
Evidence brief for policy and practice Children and young people’s mental health and domestic and family violence: What’s the link?
Every child deserves the right to grow up in a safe, happy and healthy environment. When children experience domestic and family violence (DFV), it disrupts that right and can have long-lasting impacts on their health and wellbeing.
This resource draws on research funded by ANROWS and led by Dr Carol Orr from The University of Western Australia to build the evidence base, for those working in policy and with children and families, about the connections between DFV and children’s mental health and wellbeing.
What is mental health?
Mental health is a state of wellbeing in which individuals realise their abilities, cope with the everyday stresses of life, work productively, and contribute to their community (World Health Organization, 2018). When children have positive mental health, they can better regulate their emotions and respond to stress.
Why is positive mental health so important?
Mental health and wellbeing exist on a continuum from well to unwell. This continuum approach to mental health and wellbeing emphasises the many opportunities to act to support improved health and minimise the likelihood that children will become unwell. There is increasing recognition of the importance of children’s mental health and wellbeing, according to the National Children’s Mental Health and Wellbeing Strategy:
Good mental health and wellbeing enables children to reach their full potential, experience fulfilling relationships, and adapt and cope with challenging circumstances. We know that mental health challenges often begin during childhood and if left unattended they can lead to poor outcomes in adulthood. Early intervention and prevention, with a focus on children and their families, is key to improving positive lifelong mental health and wellbeing outcomes. (Australian Government National Mental Health Commission, 2021, p. 3)
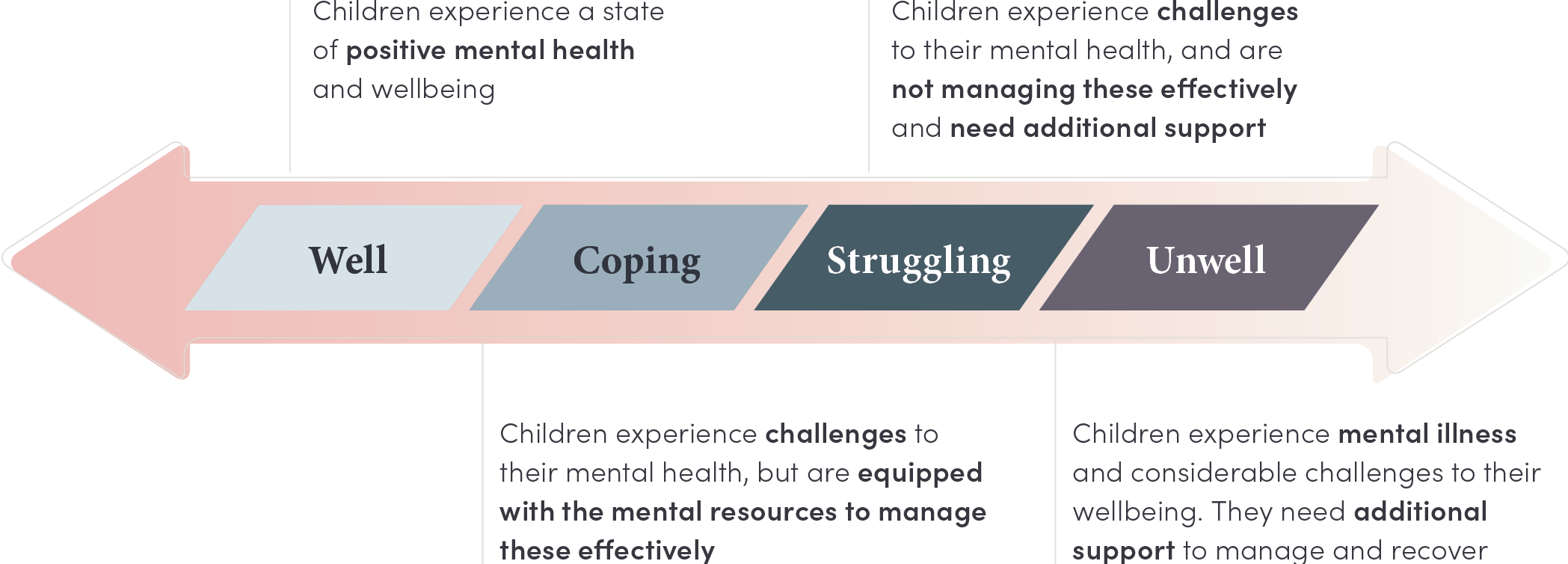
Source: Australian Government National Mental Health Commission, 2021, p. 7
What can get in the way of positive mental health for children and young people?
External factors such as poverty, housing instability and child abuse can negatively impact a child’s mental health. Increasingly, researchers are learning more about how experiencing DFV creates an ongoing stress response in a child’s brain, increasing the risk of physical and psychological illness.
What’s the link between domestic and family violence and child mental health?
DFV is one of the most prevalent stressors children can experience (Margolin & Gordis, 2000 as cited in Orr et al., 2022, p. 20). While researchers are yet to fully understand how stress contributes to ill health, emerging research points to the central role of the hypothalamic-pituitary-adrenal axis (HPA axis).
The HPA axis is an essential stress response that helps people respond appropriately to everyday stressors. Ongoing stressful events can lead to chronic activation of the HPA axis and can challenge the body’s response systems, increasing the risk for physical and psychological illness (Cohen et al., 2007; Juruena et al., 2020; Kiecolt-Glaser & Glaser, 2005; Mueller & Tronick, 2019 as cited in Orr et al., 2022, p. 19).
While some children experiencing DFV may show signs of mental health distress, others may show no apparent signs of poor mental health. Research suggests we often see children who seem unaffected by trauma as resilient, but there could be a “sleeper effect” where children only begin to struggle with their mental health years later.
Why do we need more reliable evidence about the impact of domestic and family violence on children’s mental health?
The current research on DFV and children’s mental health shows an association between DFV and mental health issues.
The research we do have is often limited due to small sample sizes, recruitment through specialist services and short study periods.
These limitations mean there is little research at a population level exploring how various mental health issues and the use of mental health services may emerge as children grow into adolescence
and adulthood.
So, what can this population-level study from Western Australia tell us?
A group of researchers looked at children born in Western Australia between 1987 and 2010. Their study used police and health records to follow children from birth to 18 years. They were specifically looking at whether the children had:
- experienced DFV (as evident in police and hospital records)
- been in contact with a mental health service
- received a mental health disorder diagnosis.
To gather this information, they used data linkage – a technique which combines information about children and their families from different records and sources.
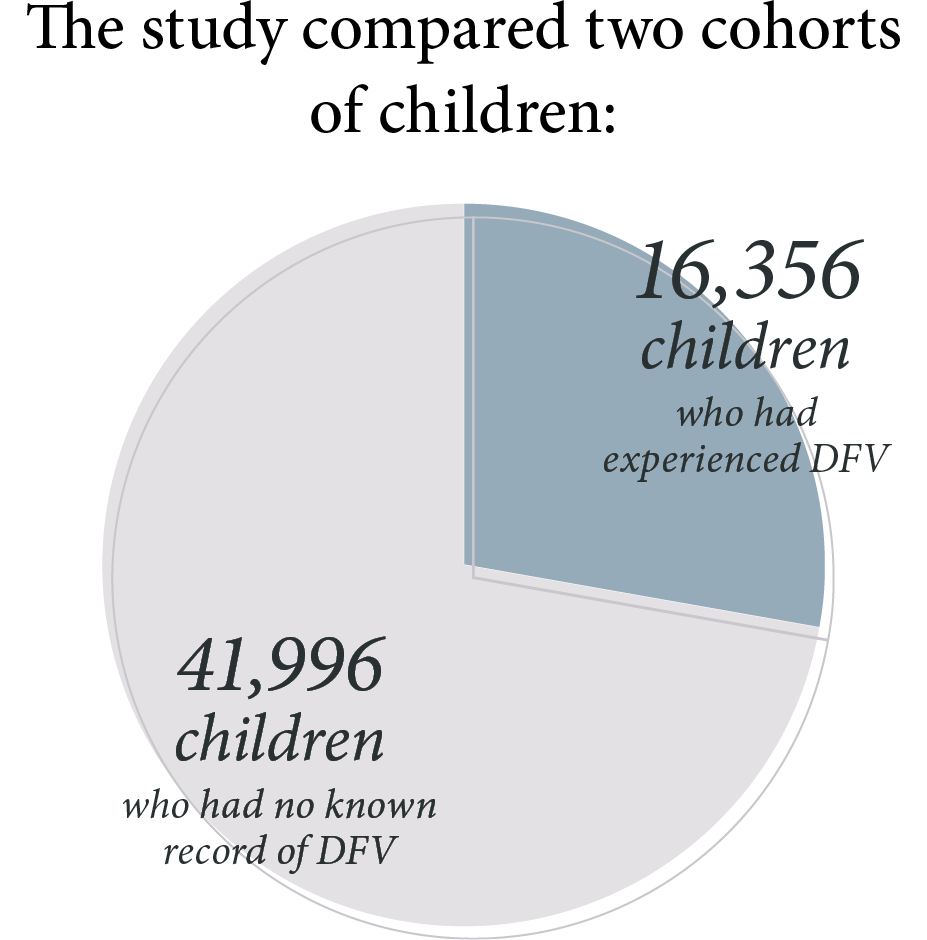
The study compared one group of children who had experienced DFV with a group with no known record of DFV. That way, researchers could identify the likelihood of mental health service contact and disorders between the two groups.
What did the study find?
The study found that children who had experienced DFV were almost five times more likely to receive treatment from a mental health service by the time they turned 18 than children who had not experienced violence (79% as opposed to 16%).
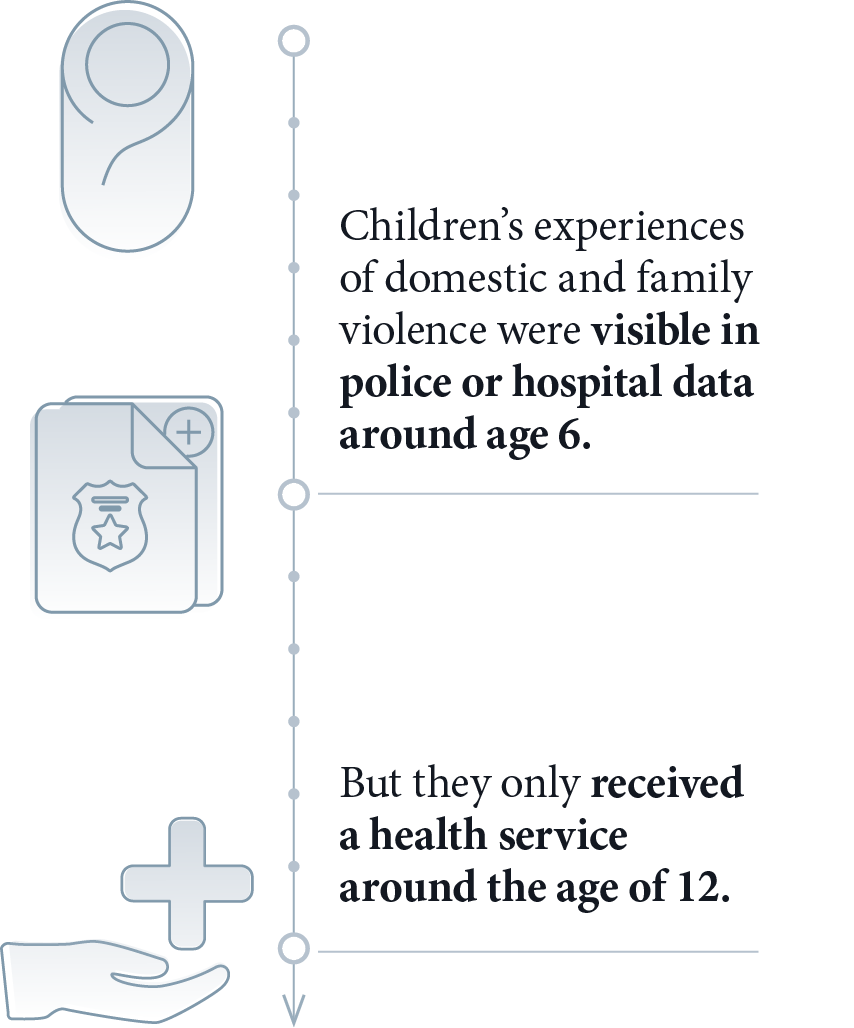
On average, children’s experiences of DFV were visible in police or hospital data around age 6. But they only received a health service around the age of 12. This finding shows a six-year gap between children’s experiences becoming known to police and health services and children receiving a mental health response.
Almost half of the children who had experienced DFV had a mother with a mental health service contact (45%). That’s more than double the number of children with no known record of DFV (21%).
What about different mental health issues?
Children who had experienced DFV were more likely to be diagnosed with many mental health issues. They were:
- 1.2 times more likely to be diagnosed with a
psychological development disorder. - 1.4 times more likely to be diagnosed with a
depressive disorder. - 1.4 times more likely to be diagnosed with
schizophrenia and psychoses. - 1.4 times more likely to be diagnosed with an
organic disorder. - 1.5 times more likely to be diagnosed with an
anxiety disorder. - 1.6 times more likely to be diagnosed with
intentional self-harm. - 1.8 times more likely to be diagnosed with a personality disorder.
- twice as likely to be diagnosed with a substance use disorder.
What can the study tell us about the needs of Aboriginal and Torres Strait Islander children?
The study also explored the relative mental health risks for Aboriginal and Torres Strait Islander children and young people. This part of the study compared the diagnoses of First Nations children who had experienced violence to those who had not. It found that Aboriginal and Torres Strait Islander children who had experienced DFV were more likely to intentionally self-harm. Aboriginal and Torres Strait Islander children who had not experienced DFV did not have this increased risk.
A 2020 report led by Pat Dudgeon described Aboriginal and Torres Strait Islander suicide as a “significant and growing crisis which requires systemic whole-of-community and whole-of-government Indigenous-led prevention” (Dudgeon et al., 2020, p. 9). Evidence highlighting the relationship between DFV and intentional self-harm among children and young people further emphasises calls for Aboriginal and Torres Strait Islander-led responses to violence and social and emotional wellbeing.
What does this mean for policy and practice?
While child mental health disorders are a serious issue, childhood also presents the most significant opportunity for intervention.
Children experiencing DFV need access to holistic services to address multiple needs such as domestic violence, disability, child mental health and maternal mental health. While holistic services are critical, we must minimise the potentially negative impacts of having multiple services working in disconnected ways with children and families. Collaboration is key to effective care.
Programs and services must be culturally safe and trauma informed. This includes supporting all people working with children and families to be curious about children’s experiences of DFV, and intervening early to support children’s mental health and wellbeing.
If you’re working with children and young people or their families:
- Be curious about their experiences of DFV and their mental health and wellbeing.
- Understand that DFV is a known stressor which can negatively affect a child’s developing mind – including their mental health and wellbeing.
- If a young child is experiencing violence but not showing signs of mental ill health, don’t wait to link them in with mental health services. Earlier support may minimise the likelihood of children struggling or becoming unwell.
- Be curious, not judgemental, about how children and young people may use alcohol and other substances and what motivates them to use substances. The twofold risk of substance use disorder this study found among children who had experienced DFV could reflect the ways young people use substances to cope with the effects of physical and emotional trauma.
- Support parents, caregivers and other important people in a child’s or young person’s life to understand the importance of mental health and wellbeing and the adverse effects DFV can have on these.
- Don’t hold victims and survivors accountable for leaving violence. Acknowledge that many factors interfere with a woman’s ability to leave violence. Leaving can increase the risk to both a woman’s and her children’s safety. At the same time, financial and housing barriers can make leaving impossible, especially if women have children with additional needs such as disability or mental ill health.
- Know that when there is DFV, both mothers and children can experience mental health issues and will need appropriate support. Don’t blame victims and survivors for the effects of DFV.
Where can I go to learn more?
Previous ANROWS research found that fathers, including stepfathers and new partners, who use violence are often invisible in child protection practice. Read the
Invisible practices: Working with fathers who use violence – Practice guide[1] to learn more about the Safe & Together™ model. This model has been designed for practitioners working with families to keep children safe. It encourages practitioners to partner with the non-offending parent while holding the person using violence accountable.
You can also find a range of resources about child-aware practice when working with families experiencing DFV via Emerging Minds.[2] This website also hosts a short online course.[3]
References
Australian Government National Mental Health Commission. (2021).
The National Children’s Mental Health and Wellbeing Strategy. https://www.mentalhealthcommission.gov.au/getmedia/e369a330-f8c3-4b9e-ab76-7a428f9ff0e3/national-childrens-mental-health-and-wellbeing-strategy-report-25oct2021.
Dudgeon, P., Bray, A., Smallwood, G., Walker, R., & Dalton, T. (2020).
Wellbeing and healing through connection and culture. Lifeline Australia.
https://doi.org/10.6084/m9.figshare.14036774
Orr, C., Sims, S., Fisher, C., O’Donnell, M., Preen, D., Glauert, R., Milroy, H., & Garwood, S. (2022).
Investigating the mental health of children exposed to domestic and family violence through the use of linked police and health records
(Research report, 09/2022). ANROWS.
World Health Organization. (2018).
Mental health: Strengthening our response.
https://www.who.int/news-room/fact-sheets/detail/mental-health-strengthening-our-response
Suggested citation
Australia’s National Research Organisation for Women’s Safety. (2022).
Children and young people’s mental health and domestic and family violence: What’s the link?
[Evidence brief for policy and practice]. ANROWS.
Endnotes
Every child deserves the right to grow up in a safe, happy and healthy environment. When children experience domestic and family violence (DFV), it disrupts that right and can have long-lasting impacts on their health and wellbeing.
This resource draws on research funded by ANROWS and led by Dr Carol Orr from The University of Western Australia to build the evidence base, for those working in policy and with children and families, about the connections between DFV and children’s mental health and wellbeing.
What is mental health?
Mental health is a state of wellbeing in which individuals realise their abilities, cope with the everyday stresses of life, work productively, and contribute to their community (World Health Organization, 2018). When children have positive mental health, they can better regulate their emotions and respond to stress.
Why is positive mental health so important?
Mental health and wellbeing exist on a continuum from well to unwell. This continuum approach to mental health and wellbeing emphasises the many opportunities to act to support improved health and minimise the likelihood that children will become unwell. There is increasing recognition of the importance of children’s mental health and wellbeing, according to the National Children’s Mental Health and Wellbeing Strategy:
Good mental health and wellbeing enables children to reach their full potential, experience fulfilling relationships, and adapt and cope with challenging circumstances. We know that mental health challenges often begin during childhood and if left unattended they can lead to poor outcomes in adulthood. Early intervention and prevention, with a focus on children and their families, is key to improving positive lifelong mental health and wellbeing outcomes. (Australian Government National Mental Health Commission, 2021, p. 3)
Source: Australian Government National Mental Health Commission, 2021, p. 7
What can get in the way of positive mental health for children and young people?
External factors such as poverty, housing instability and child abuse can negatively impact a child’s mental health. Increasingly, researchers are learning more about how experiencing DFV creates an ongoing stress response in a child’s brain, increasing the risk of physical and psychological illness.
What’s the link between domestic and family violence and child mental health?
DFV is one of the most prevalent stressors children can experience (Margolin & Gordis, 2000 as cited in Orr et al., 2022, p. 20). While researchers are yet to fully understand how stress contributes to ill health, emerging research points to the central role of the hypothalamic-pituitary-adrenal axis (HPA axis).
The HPA axis is an essential stress response that helps people respond appropriately to everyday stressors. Ongoing stressful events can lead to chronic activation of the HPA axis and can challenge the body’s response systems, increasing the risk for physical and psychological illness (Cohen et al., 2007; Juruena et al., 2020; Kiecolt-Glaser & Glaser, 2005; Mueller & Tronick, 2019 as cited in Orr et al., 2022, p. 19).
While some children experiencing DFV may show signs of mental health distress, others may show no apparent signs of poor mental health. Research suggests we often see children who seem unaffected by trauma as resilient, but there could be a “sleeper effect” where children only begin to struggle with their mental health years later.
Why do we need more reliable evidence about the impact of domestic and family violence on children’s mental health?
The current research on DFV and children’s mental health shows an association between DFV and mental health issues.
The research we do have is often limited due to small sample sizes, recruitment through specialist services and short study periods.
These limitations mean there is little research at a population level exploring how various mental health issues and the use of mental health services may emerge as children grow into adolescence
and adulthood.
So, what can this population-level study from Western Australia tell us?
A group of researchers looked at children born in Western Australia between 1987 and 2010. Their study used police and health records to follow children from birth to 18 years. They were specifically looking at whether the children had:
- experienced DFV (as evident in police and hospital records)
- been in contact with a mental health service
- received a mental health disorder diagnosis.
To gather this information, they used data linkage – a technique which combines information about children and their families from different records and sources.
The study compared one group of children who had experienced DFV with a group with no known record of DFV. That way, researchers could identify the likelihood of mental health service contact and disorders between the two groups.
What did the study find?
The study found that children who had experienced DFV were almost five times more likely to receive treatment from a mental health service by the time they turned 18 than children who had not experienced violence (79% as opposed to 16%).
On average, children’s experiences of DFV were visible in police or hospital data around age 6. But they only received a health service around the age of 12. This finding shows a six-year gap between children’s experiences becoming known to police and health services and children receiving a mental health response.
Almost half of the children who had experienced DFV had a mother with a mental health service contact (45%). That’s more than double the number of children with no known record of DFV (21%).
What about different mental health issues?
Children who had experienced DFV were more likely to be diagnosed with many mental health issues. They were:
- 1.2 times more likely to be diagnosed with a
psychological development disorder. - 1.4 times more likely to be diagnosed with a
depressive disorder. - 1.4 times more likely to be diagnosed with
schizophrenia and psychoses. - 1.4 times more likely to be diagnosed with an
organic disorder. - 1.5 times more likely to be diagnosed with an
anxiety disorder. - 1.6 times more likely to be diagnosed with
intentional self-harm. - 1.8 times more likely to be diagnosed with a personality disorder.
- twice as likely to be diagnosed with a substance use disorder.
What can the study tell us about the needs of Aboriginal and Torres Strait Islander children?
The study also explored the relative mental health risks for Aboriginal and Torres Strait Islander children and young people. This part of the study compared the diagnoses of First Nations children who had experienced violence to those who had not. It found that Aboriginal and Torres Strait Islander children who had experienced DFV were more likely to intentionally self-harm. Aboriginal and Torres Strait Islander children who had not experienced DFV did not have this increased risk.
A 2020 report led by Pat Dudgeon described Aboriginal and Torres Strait Islander suicide as a “significant and growing crisis which requires systemic whole-of-community and whole-of-government Indigenous-led prevention” (Dudgeon et al., 2020, p. 9). Evidence highlighting the relationship between DFV and intentional self-harm among children and young people further emphasises calls for Aboriginal and Torres Strait Islander-led responses to violence and social and emotional wellbeing.
What does this mean for policy and practice?
While child mental health disorders are a serious issue, childhood also presents the most significant opportunity for intervention.
Children experiencing DFV need access to holistic services to address multiple needs such as domestic violence, disability, child mental health and maternal mental health. While holistic services are critical, we must minimise the potentially negative impacts of having multiple services working in disconnected ways with children and families. Collaboration is key to effective care.
Programs and services must be culturally safe and trauma informed. This includes supporting all people working with children and families to be curious about children’s experiences of DFV, and intervening early to support children’s mental health and wellbeing.
If you’re working with children and young people or their families:
- Be curious about their experiences of DFV and their mental health and wellbeing.
- Understand that DFV is a known stressor which can negatively affect a child’s developing mind – including their mental health and wellbeing.
- If a young child is experiencing violence but not showing signs of mental ill health, don’t wait to link them in with mental health services. Earlier support may minimise the likelihood of children struggling or becoming unwell.
- Be curious, not judgemental, about how children and young people may use alcohol and other substances and what motivates them to use substances. The twofold risk of substance use disorder this study found among children who had experienced DFV could reflect the ways young people use substances to cope with the effects of physical and emotional trauma.
- Support parents, caregivers and other important people in a child’s or young person’s life to understand the importance of mental health and wellbeing and the adverse effects DFV can have on these.
- Don’t hold victims and survivors accountable for leaving violence. Acknowledge that many factors interfere with a woman’s ability to leave violence. Leaving can increase the risk to both a woman’s and her children’s safety. At the same time, financial and housing barriers can make leaving impossible, especially if women have children with additional needs such as disability or mental ill health.
- Know that when there is DFV, both mothers and children can experience mental health issues and will need appropriate support. Don’t blame victims and survivors for the effects of DFV.
Where can I go to learn more?
Previous ANROWS research found that fathers, including stepfathers and new partners, who use violence are often invisible in child protection practice. Read the
Invisible practices: Working with fathers who use violence – Practice guide[1] to learn more about the Safe & Together™ model. This model has been designed for practitioners working with families to keep children safe. It encourages practitioners to partner with the non-offending parent while holding the person using violence accountable.
You can also find a range of resources about child-aware practice when working with families experiencing DFV via Emerging Minds.[2] This website also hosts a short online course.[3]
References
Australian Government National Mental Health Commission. (2021).
The National Children’s Mental Health and Wellbeing Strategy. https://www.mentalhealthcommission.gov.au/getmedia/e369a330-f8c3-4b9e-ab76-7a428f9ff0e3/national-childrens-mental-health-and-wellbeing-strategy-report-25oct2021.
Dudgeon, P., Bray, A., Smallwood, G., Walker, R., & Dalton, T. (2020).
Wellbeing and healing through connection and culture. Lifeline Australia.
https://doi.org/10.6084/m9.figshare.14036774
Orr, C., Sims, S., Fisher, C., O’Donnell, M., Preen, D., Glauert, R., Milroy, H., & Garwood, S. (2022).
Investigating the mental health of children exposed to domestic and family violence through the use of linked police and health records
(Research report, 09/2022). ANROWS.
World Health Organization. (2018).
Mental health: Strengthening our response.
https://www.who.int/news-room/fact-sheets/detail/mental-health-strengthening-our-response
Suggested citation
Australia’s National Research Organisation for Women’s Safety. (2022).
Children and young people’s mental health and domestic and family violence: What’s the link?
[Evidence brief for policy and practice]. ANROWS.