
RESEARCH REPORT Investigating the mental health of children exposed to domestic and family violence through the use of linked police data and health records
Dr Carol Orr
Research Fellow, The School of Population and Global Health,
The University of Western Australia
Scott Sims
Biostatistician, The School of Population and Global Health,
The University of Western Australia
Professor Colleen Fisher
Head of School, The School of Population and Global Health,
The University of Western Australia
Associate Professor Melissa O’Donnell
Deputy Director, Australian Centre for Child Protection,
The University of South Australia
Professor David Preen
Chair in Public Health, The School of Population and Global Health,
The University of Western Australia
Associate Professor Rebecca Glauert
Principal Research Fellow, The School of Population and Global Health,
The University of Western Australia
Professor Helen Milroy
Stan Perron Professor Child and Adolescent Psychiatry Perth Children’s Hospital and
The University of Western Australia
Dr Shae Garwood
Manager, Research, Advocacy & Prevention Innovation & Strategy,
Anglicare WA
Research Report
Issue 10 | July 2022
ANROWS acknowledgement
This material was produced with funding from the Australian Government and the Australian state and territory governments. Australia’s National Research Organisation for Women’s Safety (ANROWS) gratefully acknowledges the financial and other support it has received from these governments, without which this work would not have been possible. The findings and views reported in this paper are those of the authors and cannot be attributed to the Australian Government, or any Australian state or territory government.
ANROWS Acknowledgement of Country
ANROWS acknowledges the Traditional Owners of the land across Australia on which we work and live. We pay our respects to Aboriginal and Torres Strait Islander Elders past, present and future, and we value Aboriginal and Torres Strait Islander histories, cultures and knowledge. We are committed to standing and working with Aboriginal and Torres Strait Islander peoples, honouring the truths set out in the Warawarni-gu Guma Statement.
Peer review process
The quality of ANROWS publications is ensured through a rigorous peer review process that is consistent with the principles of the Committee on Publication Ethics (COPE) Ethical Guidelines for Peer Review. This report has been assessed by at least two peer reviewers with relevant academic expertise.
© ANROWS 2022
With the exception of the ANROWS branding, content provided by third parties, and any material protected by a trademark, all material presented in this publication is licensed under a Creative Commons Attribution-NonCommercial 3.0 Australia (CC BY-NC 3.0 AU) licence.

The full licence terms are available at creativecommons.org/licenses/by-nc/3.0/au/legalcode
Published by
Australia’s National Research Organisation for Women’s Safety Limited (ANROWS)
PO Box Q389, Queen Victoria Building, NSW 1230 | www.anrows.org.au | Phone +61 2 8374 4000
ABN 67 162 349 171
ISBN: 978-1-922645-34-0 (paperback)
ISBN: 978-1-922645-35-7 (PDF)
Please note that there is the potential for minor revisions of this report.
Please check the online version at www.anrows.org.au for any amendment.
This report addresses work covered in the ANROWS research project RP.20.05 “Investigating the mental health of children exposed to domestic and family violence through the use of linked police and health records”. Please consult the ANROWS website for more information on this project.
ANROWS research contributes to the six National Outcomes of the National Plan to Reduce Violence against Women and their Children 2010–2022. This research addresses National Plan Outcome 4: Services meet the needs of women and their children experiencing violence.
Suggested citation:
Orr, C ., Sims, S., Fisher, C., O’Donnell, M., Preen, D., Glauert, R., Milroy, H., & Garwood, S. (2022). Investigating the mental health of children exposed to domestic and family violence through the use of linked police and health records (Research report, 10/2022). ANROWS.

The University of Western Australia
35 Stirling Hwy
Crawley WA 6009
Author acknowledgement
The authors would like to thank the Linkage, Data Outputs and Research Data Services teams at the Western Australian Data Linkage Branch, in particular the Data Custodians of the Midwives Notification System, Hospital Morbidity Data System, Mental Health Information System, Birth Registration, Death Registration, IDEA Database, Western Australia Register of Developmental Anomalies, Department of Communities – Child Protection and Family Support data, and the Western Australia Police Force. We would also like to thank Wungening Aboriginal Corporation and our community and consumer representative groups. We extend our gratitude to the people of Western Australia for the use of their de-identified administrative data.
This report does not necessarily reflect the views of the government departments involved in this research and any errors of omission or commission are the responsibility of the researchers.
Acknowledgement of lived experiences of violence
ANROWS acknowledges the lives and experiences of the women and children affected by domestic, family and sexual violence who are represented in this report. We recognise the individual stories of courage, hope and resilience that form the basis of ANROWS research.
ANROWS acknowledges that children and young people living in homes where domestic and family violence (DFV) is present are not simply “exposed” to DFV – they are experiencing it. There are no circumstances in which children and young people are exposed to DFV and are not also being impacted by this violence. Therefore, ANROWS will always default to using “experienced DFV” instead of “were exposed to DFV” or “witnessed DFV”. This language aligns with the National Plan to End Violence Against Women and Children (due for finalisation in 2022), which recognises that children experience DFV as victims in their own right, and also seeks to honour the voices of victims and survivors who have felt minimised, erased or unacknowledged as childhood survivors.
Please note that in this report, the authors have chosen to use the term “exposed to DFV”, and have provided a rationale for this choice in the “Definitions and key concepts” section.
Caution: Some people may find parts of this content confronting or distressing. Recommended support services include 1800RESPECT (1800 737 732), Lifeline (13 11 14) and, for Aboriginal and Torres Strait Islander people, 13YARN (13 92 76).
Acronyms
Acronym
Definition
ABS
Australian Bureau of Statistics
AEDC
Australian Early Development Census
AIFS
Australian Institute of Family Studies
AIHW
Australian Institute of Health and Welfare
ANROWS
Australia’s National Research Organisation for Women’s Safety
ARIA
Accessibility/Remoteness Index of Australia
CALD
Culturally and linguistically diverse
CI
Confidence interval
DSM-5
Diagnostic and Statistical Manual of Mental Disorders (Fifth Edition)
DFV
Domestic and family violence
EDDC
Emergency Department Data Collection
HMDC
Hospital Morbidity Data Collection
HPA axis
Hypothalamic-pituitary-adrenal axis
ICD
International Classifications of Disease
ICD-9
International Classifications of Disease Ninth Edition
ICD-10AM
International Classifications of Disease 10th Edition Australian Modification
IDEA
Intellectual Disability Exploring Answers
IMS
Incident Management System
MHIS
Mental Health Information System
PTSD
Post-traumatic stress disorder
RANZCP
Royal Australian and New Zealand College of Psychiatrists
SD
Standard deviation
SAS
Statistical Analysis System
SEIFA
Socioeconomic Indexes for Areas
SES
Socioeconomic status
SNAICC
Secretariat of National Aboriginal and Islander Child Care
UN
United Nations
UNICEF
United Nations Children’s Fund
VIF
Variance inflation factors
WARDA
Western Australian Register of Developmental Anomalies
WHO
World Health Organization
Definitions and concepts
Concept
Definition
Domestic and
family violence
Domestic and family violence (DFV) refers to the threat of, or acts of, violence or abuse of a physical, non-physical and/or sexual nature between people who are currently or have previously been in an intimate relationship (Council of Australian Governments, 2011). The central component of DFV is an ongoing pattern of behaviour aimed at controlling a person through fear by use of violent and/or threatening behaviour (Council of Australian Governments, 2011). The acts can be both criminal and
non-criminal.
Women subjected
to DFV
Debate exists in regard to the use of the terms “victim” and/or “survivor”. Due to the stigma attached, those living with DFV frequently object to the use of either term (Papendick et al., 2017). As this report uses population linked administrative data, the individual journey of those abused, whether they have started the recovery process or not, and their preference for the use of the term “victim” and/or “survivor” is unknown. Therefore, the term “subjected to DFV” is used throughout this report to describe a woman who has been abused by a man in the context of DFV.
Identification of DFV
This report captures DFV perpetrated by men against women. While men can also be victims of DFV perpetrated by a partner of the same or different sex (AIHW, 2018b), DFV is a gendered act that is disproportionately perpetrated by men against women (European Institute for Gender Inequality, 2017; World Health Organization [WHO], 2014). Recognising the gendered patterns of DFV does not negate the experiences of men who are subjected to DFV. It does, however, acknowledge the need to address the issue through a gendered lens. Therefore, in the context of this report, “DFV” refers to DFV perpetrated by men against women.
Perpetrator
The men who commit acts of DFV are referred to as “perpetrators”. “Perpetrator” is the term used in the National Outcome Standards for Perpetrator Interventions (National Outcome Standards; Council of Australian Governments, 2015) to describe men who commit DFV against women. While the phrase “men who use violence” is preferred by some (Heward-Belle et al., 2019) because it labels the behaviour rather than the person (Council of Australian Governments, 2015), the term “perpetrator” reinforces the serious nature of DFV. The term includes all men who commit one or more identified acts of DFV.
Child
The term “child/children” will be used to capture those under the age of 18 as used in the Children and Community Services Act 2004 (WA).
Exposure to DFV
Within the literature there is a lack of common terminology and definitions of children exposed to DFV, despite this issue being acknowledged more than 30 years ago (Fantuzzo & Lindquist, 1989). DFV literature often uses the terms “witnessed” or “exposed to” and at times they are used interchangeably (Berg et al., 2020; Howarth et al., 2016; Kitzman et al., 2003; Spilsbury et al., 2008). The term “witness” is restrictive in the context of DFV. Far from being passive observers, children experience DFV with all of their senses (Devaney, 2015). Moreover, the dichotomy of whether a child observed or overheard violence or not is too simplistic (Holden, 2003). The child may not always observe DFV; the abuse may be psychological and controlling behaviour by the perpetrator and not physically visible to the child, but they are still aware that the abuse is happening (Överlien & Hydén 2009; Swanston et al., 2014). Holden (2003) arguesthat the term “exposed to” is more inclusive of the different types of experiences of the child and does not assume that the child observed the DFV. Holden developed a taxonomy of exposure that is separated into 10 discrete categories (see Table 1). The taxonomy ranges from the child being actively involved in the DFV to the child being ostensibly unaware of it. In this report the term “exposure to DFV” will be used to ensure the capture of the child’s full experience, the scope of which is defined in
Table 1.
International Classification of Disease codes
International Classification of Disease (ICD) codes are standardised medical classification codes authorised by the World Health Organization (WHO) for the classification of diseases, injuries, health encounters, social circumstances, external causes of injury or diseases, and inpatient procedures in morbidity (health) settings. The ICD classification is used globally. Some countries, however, have modified it to better suit their needs. Within Australia, the current ICD codes have been amended to suit Australian needs and are known as the ICD-10 Australian Modification (ICD-10-AM).
Aboriginal and Torres Strait Islander
The data used in this report contained a variable that identified a combined Aboriginal and Torres Strait Islander status (see Christensen et al., 2014). Therefore, in this report, the term “Aboriginal and Torres Strait Islander” is used in preference to “Indigenous” or “Aboriginal”.
Culturally and linguistically diverse
There is considerable inconsistency in how culturally and linguistically diverse (CALD) status is defined within Australia (Pham et al., 2021). CALD can often include those born overseas, those having a parent born overseas, those whose main language spoken at home is not English, and particular religious affiliations (Australian Institute of Health and Welfare [AIHW], 2018a; Pham, 2021). The term “CALD” in this report will include those children with one or both parents born overseas, including the United Kingdom and New Zealand (AIHW, 2018a).
Disability
As a concept, disability is complex, dynamic, multidimensional and contested (WHO, 2011a). The term “disability” has divergent meanings with no national or international consensus on how it is defined. In the study contained in this report, a child was defined as having disability if they had a diagnosis for autism, intellectual disability, Down syndrome, cerebral palsy or birth defect. This definition of disability has been used in previous research (e.g. Maclean, Sims et al., 2017). However, the definition of disability used in this report is narrower than that captured in the Australian Bureau of Statistics (ABS; 2016a) due to limitations in the data.
Ecological framework
The ecological model was the conceptual framework for the study and informed data analysis. The model was introduced in the 1970s by Urie Bronfenbrenner (1977) to explain how the interactive environment affects a child’s growth and development. While the ecological model was originally used to explain children’s growth and development, an ecological approach to public health issues, such as DFV, has become a more distinctive feature of prevention and promotion in contemporary public health (Richard et al., 2011). The model is a prominent explanatory framework used by the WHO to understand the interplay of personal, situational and socio-cultural factors that influence violence against women (Ellsberg & Heise, 2005; WHO, 2022).
Mental health
The WHO (2018) defines mental health as the state of wellbeing in which an individual realises his or her own abilities, can cope with the normal stresses of life, can work productively and fruitfully, and is able to make a contribution to his or her community (WHO, 2018).
Internalising behaviours
Internalising behaviours are described as “inner-directed and generating distress in the individual” (Forns et al., 2018, p. 519). Types of internalising behaviours include anxiety, dysphoria and depression.
Externalising behaviours
Externalising behaviours are a group of behaviour problems that are “outer-directed generating discomfort and conflict in the surrounding environment” (Forns et al., 2018, p. 519). These behaviours include substance misuse, impulsivity, aggressiveness and disruptiveness.
Mental health service contact
An instance of contact or service provision by an agency to an individual which was recorded in the administrative data of the agency.
Mental health services
The collective term used in this report to represent the “agency” encompassing
mental health services (these include contacts with public community mental health services, a public or private hospital admission, and presentation for a mental health-related condition).
Table 1: A taxonomy of children’s exposure to domestic violence: Type of exposure (adapted from Holden, 2003, p. 152)
Type of exposure
Definition
Examples
Exposed prenatally
Real or imagined effects of DFV on the developing foetus
Foetus assaulted in utero; pregnant mother lived in terror; mothers perceived that the DFV during pregnancy had affected their foetus
Intervenes
The child verbally or physically attempts to stop the assault
Asks parents to stop; attempts to defend mother
Victimised
The child is verbally or physically assaulted during an incident
Child intentionally injured, accidentally hit by a thrown object, etc.
Participates
The child is forced to or “voluntarily” joins in the assaults
Coerced to participate; used as spy; joins in taunting mother
Eyewitness
The child directly observes the assault
Watches assault or is present to hear verbal abuse
Overhears
The child hears, though does not see, the assault
Hears yelling, threats or breaking of objects
Observes the initial effects
The child sees some of the immediate consequences of the assault
Sees bruises or injuries; police; ambulance; damaged property; intense emotions
Experiences the aftermath
The child faces changes in their life as a consequence of the assault
Experiences maternal depression; change in parenting; separation from father; relocation
Hears about it
The child is told or overhears conversations about the assault
Learns of the assault from mother, sibling, relative or someone else
Ostensibly unaware
The child does not know of the assault, according to the source
Assault occurred away from home or while child was away; or occurred when mother believed child was asleep
Executive summary
Background
Existing literature highlights that exposure to domestic and family violence (DFV) is associated with poorer mental health in childhood (Carter et al., 2020; Gartland et al., 2021; Herrenkohl et al., 2008; Orr, Fisher, Preen et al., 2020). However, the literature is limited by the predominant use of studies focused on a short period of time with little account given to the mental health impacts that may occur over time. Existing research has also focused on the grouping of mental health issues into internalising and externalising behaviours (Vu et al., 2016) which can restrict targeted interventions.
Additionally, there is a need to conduct research in an Australian context given the disparity in rates of both exposure to DFV (Australian Bureau of Statistics [ABS], 2016b; Orr, Preen et al., 2019) and mental illness (Al-Yaman, 2017) for Aboriginal and Torres Strait Islander children. Furthermore, Australia has a long history of migration (Collins, 2013). The most recent Australian Census (ABS, 2021a) reported that 62 per cent of Western Australians have one or both parents born overseas. Evidence is lacking on the outcomes of children who are exposed to DFV and culturally and linguistically diverse (CALD). Additionally, within Australia, 8 per cent of children under 15 have disability (ABS, 2019). The greater dependency of children with disability on carers and family support and the time spent in the family home are thought to place the child at greater risk of DFV exposure (Baldry et al., 2006). The effects of DFV exposure on children withdisability remain poorly understood (Dababnah et al., 2018).
Aim and objectives
The aim of this research was to identify the mental health service use and diagnoses of children exposed to DFV in Western Australia between 1987 and 2016.
The specific objectives were to:
1. Examine the mental health service use and trajectories of children exposed to DFV and ascertain the differences in sociodemographic characteristics and service use between exposed and non-exposed children.
2a. Identify mental health diagnosis types for children exposed to DFV compared to non-exposed children.
2b. Identify key sociodemographic and clinical characteristics predictive of mental health diagnosis and diagnosis subtypes of children with known DFV.
3. Examine differences in mental health service use and diagnosis types in Aboriginal and Torres Strait Islander children and non-Aboriginal and Torres Strait Islander children who are exposed to DFV as well as other sub-populations of children, including those from CALD backgrounds and children with disability, who are exposed to DFV.
Methods
This study comprised a population-based retrospective cohort study of children born in Western Australia between 1987 and 2010 who were exposed to DFV. Exposure to DFV was initially identified in the Western Australia Police Force Information Management System (IMS) when a child’s mother was identified (in Western Australia) as being subjected to DFV from 2004 to the end of 2008, a male perpetrator was charged for the offence and a domestic relationship indicator was recorded. There were 15,598 children born to mothers who were identified as victims of DFV in the Western Australia Police Force IMS. The children were firstly matched in a ratio of 1:3 to a non-DFV-exposed cohort of children based on month of birth, socioeconomic status (SES), Aboriginal and Torres Strait Islander status, and sex. Due to the hidden nature of DFV we also examined non-exposed children for any maternal DFV hospitalisations by interrogating the Western Australian hospitalrecords of their mothers from 1979 to 2016 (inclusive) using International Classification of Diseases (ICD) codes (WHO, 2011b). We found that 4,442 originally “non-exposed” children had a mother who had a hospitalisation indicating DFV. The children exposed to DFV were then restricted to those who were between the ages of 0 and 18 when the identified DFV occurred. This approach resulted in an exposed cohort of 16,356 and a non-exposed cohort of 41,996.
Aboriginal and Torres Strait Islander children were identified by the Western Australian Data Linkage Branch derived Aboriginal status flag. Disability was identified from three sources: 1) the child was recorded in the Western Australian Register of Developmental Anomalies (WARDA) datasets as having a birth defect or cerebral palsy; 2) intellectual disability was captured in the Intellectual Disability Exploring Answers (IDEA) database; or 3) ICD codes were used to identify disability in Hospital Morbidity Data Collection (HMDC) records. CALD children were identified from the WA Registry of Births, Deaths and Marriages where one or both parents were born overseas.
Mental health service use was defined as a child having had any mental illness-related diagnosis across the HMDC, Mental Health Information System (MHIS) and Emergency Department Data Collection (EDDC) datasets during the follow-up period. Children were followed until they reached 18 years of age, date of death or until the end of follow-up period in 2017, whichever came first. Only a child’s first mental illness-related contact after DFV (across the three data collections) was considered for modelling purposes relating to overall service contact.
Mental health diagnosis was identified across the three data collections (HMDC, EDDC and MHIS) utilising ICD codes. The diagnoses were categorised into 10 main groupings: organic disorder, substance use disorder, schizophrenia and psychoses, depressive disorder, anxiety disorder, personality disorder, psychological development disorder, intentional self-harm, other mental illness-related contacts, and mental health contact with no diagnosis recorded.
Multiple approaches to statistical analysis were undertaken.
Results
Children exposed to DFV had a statistically significant 49 per cent increased risk of mental health service contact when compared with non-exposed children. On average the children were exposed to DFV when aged 6.5 years, however, the children were, on average, aged 12.5 years at mental health service contact. Almost half of children exposed to DFV had a mother with a mental health contact (45%) – this was more than double the proportion seen in non-exposed children (21%).
Over time, children exposed to DFV had a 79 per cent chance of having a mental health contact by age 18, whereas for children not exposed to DFV, the chance of having a mental health service contact was 16 per cent by age 18.
Children exposed to DFV had a higher risk of having a diagnosis in eight of the 10 mental health subcategories compared to their non-exposed peers. This ranged from a 19 per cent increased risk in psychological development disorders (which include behavioural and emotional disorders) to a 99 per cent increased risk in substance use disorder. Only the categories “organic disorder” (including cerebral dysfunction) and “other mental illness-related contacts” showed no significant risk increase for children exposed to DFV when compared to non-exposed children.
Aboriginal and Torres Strait Islander children were overrepresented in our exposed cohort when compared to the state of Western Australia. According to the 2016 Census (ABS, 2018c), only 7 per cent of people under 18 in Western Australia were Aboriginal and Torres Strait Islander compared to 62 per cent of children in our exposed group. Possible reasons as to why Aboriginal and Torres Strait Islander children were overrepresented in this cohort are explored in subsequent sections discussing the study’s findings and its strengths and limitations. For Aboriginal and Torres Strait Islander children exposed to DFV, being born to a mother aged under 30 was associated with a decreased risk of mental health service contact of 18 per cent to 25 per cent, compared to those with an older mother. However, for non-exposed Aboriginal and Torres Strait Islander children, maternal age was not associated with mental health service contact.
For children with disability who were exposed to DFV, being born pre-term was associated with a 23 per cent increased risk of mental health service contact when compared to DFV-exposed children born at term. However, being born early was not a risk for mental health service contact in children with disability who were not exposed to DFV.
Due to limitations in the data, outcomes for CALD children were unable to be investigated.
Strengths and limitations
The main strength of the research was the use of population-level administrative data, linked across multiple agencies, at both the child and parent level to investigate the mental health of children exposed to DFV. The use of linked police and hospital data to identify DFV exposure enabled investigations of high-risk groups not captured in previous mental health research.
While the use of linked administrative data provides many advantages, there are some limitations that should be noted. The children identified as exposed to DFV in this report were only recognised because of the mother’s involvement in police or hospital services. As such, the data may be subject to selection bias, capturing mainly physical cases of DFV, and may underestimate the impact of DFV exposure on children’s mental health outcomes due to the fact that not all children exposed to DFV were captured. It is therefore likely that the estimates presented in this report are conservative estimates of the association between DFV and the mental health of children exposed to DFV.
Furthermore, Aboriginal and Torres Strait Islander children were overrepresented in the cohort. This could be, in part, due to the police records of DFV requiring a charge to be made against the man; there is evidence to suggest that the likelihood of being charged for DFV is increased by a variety of socioeconomic and demographic characteristics, such as Aboriginal status (Cunneen, 2010; Jeffries & Bond, 2015). Additionally, DFV was identified in maternal hospital records where Aboriginal and Torres Strait Islander women are overrepresented (Orr, Preen et al., 2019).
The capture of mental illness in children was identified by public and private hospitalisations, emergency department (ED) attendance and public outpatient mental health services. Many children with mental illness will not be identified in these data.
Implications for policy and practice
DFV exposure is associated with an increased risk of mental health service contact and diagnosis of mental illness. Early intervention is required. Many children exposed to DFV are not engaged in mental health services until years after the exposure. Additionally, the findings add further support for the need for a dedicated standalone national response and strategy for the mental health of children exposed to DFV (Australian Government, 2021).
Children exposed to DFV often live with complex issues such as maternal mental illness and disability. Therefore, services to support these children must be well resourced and holistically focused with collaborative, multidisciplinary teams and cross-agency collaboration that provides continuity of care for children and their families with multiple and complex issues.
To support children and families, it is important that mental health clinicians are aware of trauma, including DFV exposure, during childhood. Clinicians need to have knowledge of DFV and its implications for mental health as well as the ability to appropriately and safely respond to children exposed to DFV (McTavish et al., 2016). These skills need to be taught to clinicians during their training and offered as ongoing professional development to enable clinicians to stay abreast of contemporary developments. At present DFV training is not part of the mandatory suite of training across Western Australian health services. A national approach should be taken to ensure that all registered and non-registered staff within public, private and NGO health services are provided with DFV training.
Aboriginal and Torres Strait Islander peoples were overrepresented in the exposed cohort. Such overrepresentation reaffirms calls from Aboriginal and Torres Strait Islander communities that Aboriginal and Torres Strait Islander peoples should receive sufficient investment to develop policies and programs to support Aboriginal and Torres Strait Islander children.
Children exposed to DFV are not engaged in mental health services until years after exposure. To best support children exposed to DFV, early intervention is required. These children and their families are in contact with multiple agencies that may include education, health, police and child protection, and each provides a potential point of intervention. As such, it is imperative that these agencies, along with children’s mental health services, are embedded in, and part of, a broader collaborative, multiagency and multidisciplinary response to DFV, and are adapted to “fit” with the existing local response to DFV and avoid unwarranted duplication of services.
To support service engagement and reduce the re-traumatisation of children exposed to DFV, service responses must be trauma-informed and culturally responsive and secure.
Exposure to DFV is associated with an increased risk of mental health disorders in children. Our findings highlight the importance of the continuation of collective prevention efforts nationally and in each jurisdiction to reduce and eradicate DFV.
Directions for future research
There is a substantial period of time between children’s exposure to DFV and their contact with mental health services. Early access to mental health services is important for children as it can reduce the long-term impact of mental illness (MacDonald et al., 2018). Therefore, it is imperative that future research investigates factors associated with delay in service contact for children exposed to DFV as a priority.
It is acknowledged that children with mental health issues are more likely to have mental health issues in adulthood (Kessler et al., 2005; Ravens-Sieberer et al., 2015). Future research is needed to investigate the mental health of the children exposed to DFV into their adulthood. As young people with complex needs are at greater risk of “falling thorough the gaps” in care transition to adult services (Singh, 2009), attention to those exposed to DFV is needed.
There is a need for research driven by Aboriginal and Torres Strait Islander peoples on the mental health of Aboriginal and Torres Strait Islander children given the disproportionate exposure to DFV of these children. The findings contained in this report have the potential to be a stepping stone from which a holistic, culturally appropriate program of research can be developed.
To gain a greater understanding of the effect exposure to DFV has on children’s mental health, further research is required utilising multiple sources of linked data to identify both DFV and mental illness. The linked data should be complemented by combining data from population-based surveys, longitudinal surveys and social indicators (Hertzman & Williams, 2009). This multiple source approach would largely overcome the limitations of using each source separately and benefit from the strengths of each.
Conclusion
Findings from this research have shown that exposure to DFV in childhood is associated with an increased risk of mental health service contact and mental health diagnosis during childhood. The use of population-level linked administrative data has enabled the identification of sociodemographic characteristics that are associated with mental health service contact and diagnosis categories in children exposed to DFV. Additionally, the longitudinal data has provided a picture of mental health service contact over time for Western Australian children exposed to DFV. The research also offers new insights into the impact DFV has on Aboriginal and Torres Strait Islander children and children with disability.
Introduction
This report outlines the findings of a retrospective cohort study that used linked de-identified administrative data. The aim of the study was to identify the mental health outcomes of children born in Western Australia who were exposed to domestic and family violence (DFV).
Context for research
Domestic and family violence in Australia
It is difficult to accurately identify the extent of DFV in the Australian population. By their nature DFV incidents often occur at home or in other private spaces – “behind closed doors” – and are often concealed and denied by both the perpetrator and those subjected to the violence (Australian Institute of Health and Welfare [AIHW], 2018b; Phillips & Vandenbroek, 2014). The ability of data sources to measure DFV is dependent on the victim’s perception of DFV, their willingness to disclose and/or how the incident is reported (Australian Bureau of Statistics [ABS], 2017a). Global estimates of DFV suggest that almost 33 per cent of women who have been in an intimate partner relationship have experienced physical or sexual violence by an intimate partner in their lifetime (World Health Organisation [WHO], 2020a). Within Australia, DFV perpetrated by a current or former intimate partner is a widespread issue with a lifetime prevalence of 25 per cent(ABS, 2017a). The Australian Personal Safety Survey reports data on women who have been subject to DFV perpetrated by a partner in the previous 12 months. Rates of DFV have remained relatively stable over the past decade, with a slight increase in the latest (2016) survey report: 1.5 per cent of the population were subjected to DFV in 2005 and 2012, increasing to 1.7 per cent in 2016 (ABS, 2017a). DFV occurs at high rates among Aboriginal and Torres Strait Islander women (ABS, 2016b), with 10 per cent of Aboriginal and Torres Strait Islander women informing the 2015 National Aboriginal and Torres Strait Islander Social Survey that they had been victims of DFV by an intimate partner or a family member in the preceding 12 months (ABS, 2016b).
Aboriginal and Torres Strait Islander peoples hold distinctive rights as Australia’s First Peoples, set out in international law (Australian Human Rights Commission, 2015). Additionally, in 2009, Australia gave its formal support to the United Nations Declaration on the Rights of Indigenous People. However, despite these distinctive rights and as a result of colonisation and systemic racism, Aboriginal and Torres Strait Islander communities are considered among the most vulnerable groups in Australia (Australian Human Rights Commission, 2015). The National Plan to Reduce Violence against Women and their Children 2010–2022 (Council of Australian Governments, 2011) acknowledges the disproportionate rates of DFV experienced by Aboriginal and Torres Strait Islander women as a national priority. DFV is not part of traditional Aboriginal and Torres Strait Islander cultures (Blagg et al., 2020; Our Watch, 2018; Wilson et al.,2017). The disproportionate rates largely stem from deep and complex issues around dispossession and intergenerational trauma resulting from the legacy of colonisation, including systemic racism and forced removal of children (Secretariat of National Aboriginal and Islander Child Care [SNAICC], 2017). As part of this study, we explored rates of DFV and mental health disorders among both Aboriginal and Torres Strait Islander women and children and non-Indigenous women and children. In understanding the rates at which different groups experience DFV and mental ill health, research can better inform recommendations for future policy and practice including resource distribution and future research priorities.
Help-seeking by women
The most recent Australian Personal Safety Survey highlighted that around half of women (46%) who are subjected to DFV do not disclose the abuse (ABS, 2017a). A multitude of reasons have been identified: stigma, fear, lack of a safe place to disclose (García-Moreno et al., 2005; Keeling & Fisher, 2015), or believing they can deal with it themselves or that it is not serious enough to seek help (ABS, 2017a). There is also fear of child removal, a particular concern for Aboriginal and Torres Strait Islander women (Australia’s National Research Organisation for Women’s Safety [ANROWS], 2020a). Of the Australian women who do seek assistance, 53 per cent reportedly seek help from a health professional (33% from a general practitioner and 20% from another health professional) and 17 per cent from police (ABS, 2017a).
Children’s exposure to DFV
Children’s exposure to DFV is a prominent human rights issue. The United Nations Convention on the Rights of the Child (United Nations General Assembly, 1989) states that children have a universal right to live free from all forms of violence, including exposure to DFV. As a signatory to this Convention, Australia has international obligations to protect children from exposure to DFV, including acting to prohibit, prevent and respond to DFV through legislative, judicial, social and educational measures. The most recent report to the UN Committee on the Rights of the Child (Australian Human Rights Commission, 2018) on Australia’s implementation of children’s rights recommended the Australian Government increases prevention measures and responses to DFV that address its distinct impacts on children.
Domestic and family violence exposure and child mental health
Due to the hidden nature of DFV and the stigma attached, it is difficult to ascertain the prevalence of children’s exposure to DFV. The Australian Personal Safety Survey (ABS, 2017a) reported that 11 per cent of adult respondents had witnessed violence against their mother by their mother’s partner before the age of 15. Additionally, 49 per cent of the women identified in the survey data as being assaulted by their current partner reported that they had children in their care at the time, with the child hearing or seeing the violence (ABS, 2017a). Research by Indermaur (2001) has suggested that one in four young Australians (12 to 20 years) have been exposed to at least one incident of DFV against their mother or carer. This figure rises to 42 per cent among Aboriginal young people (12 to 20 years; Indermaur, 2001).
Exposure to DFV in childhood has been associated with poor mental health (e.g. Hultmann et al., 2020; Vu et al., 2016). However, much of the literature is from outside of Australia with little account given to the impacts that may occur over time, and more comprehensive evidence is needed. The use of longitudinal linked administrative data provides a means to gain a greater understanding of the long-term impact of DFV exposure on children’s mental health. Poor mental health is a public health concern, and it is estimated that one in seven Australian children aged 4 to 17 years (Goodsell et al., 2017) and almost one in four Aboriginal children aged 5 to 10 years (Shepherd et al., 2017) have a mental health disorder.
Call for research
Authors of this report undertook a “priority setting partnership” process involving those with lived experience, support people and DFV service providers (Fisher et al., 2016) in order to identify community priorities for DFV research. The partnership highlighted that researching the outcomes of children exposed to DFV was a top priority. Additionally, a recent Australian Government report (AIHW, 2018b) highlighted that there are limited data available on the experiences of children exposed to DFV and noted that data sources such as police data and longitudinal data would contribute to a more comprehensive picture of those exposed and subjected to DFV. Additionally, Australia’s National Research Agenda to Reduce Violence against Women and their Children: ANRA 2020–2022 (ANROWS, 2020b) highlights the need to investigate the short- and long-term emotional and psychological impacts of DFV on children as a priority.Furthermore, the National Agreement on Closing the Gap (Commonwealth of Australia. Department of the Prime Minister and Cabinet, 2021) highlights a reduction in incidents of DFV for Aboriginal and Torres Strait Islander families as a key target and highlights the need to explore data development to measure and report the impact of DFV on children.
Study setting
Western Australia is a geographically large state within Australia covering 2.5 million square kilometres. In the 2016 Australian Census the population of Western Australia was almost 2.5 million, with 1.9 million (76%) people residing in the Greater Perth area (ABS, 2021a), an area of almost 6,500 square kilometres. The Western Australian population has a median age of 36 years (ABS, 2017b), with 23 per cent of the population comprised of children 0 to 18 years of age (ABS, 2017c), and 3 per cent of the population is Aboriginal and Torres Strait Islander (ABS, 2021a). A quarter of Aboriginal and Torres Strait Islander peoples in Western Australia reside in very remote locations, with 40 per cent living in major cities. This is in contrast to 80 per cent of non-Aboriginal and Torres Strait Islander Western Australians who live in major cities (ABS, 2017d). The most recently available data has shown the Western Australian population to be representativeof the Australian national population on key sociodemographic, health and economic indicators (Clark et al., 2010).
Aim and objectives
Aim
The aim of this research was to identify the mental health service use and diagnoses of children exposed to DFV in Western Australia between 1987 and 2016.
Objectives
The specific objectives were to:
1. Examine the mental health service use and trajectories of children exposed to DFV and ascertain the differences in sociodemographic characteristics and service use between exposed and non-exposed children.
2a. Identify the mental health diagnosis types for children exposed to DFV compared to non-exposed children.
2b. Identify key sociodemographic and clinical characteristics predictive of mental health diagnosis and diagnosis subtypes of children with known DFV.
3. Examine differences in mental health service use and diagnosis types in Aboriginal and Torres Strait Islander children and non-Aboriginal and Torres Strait Islander children who are exposed to DFV as well as other sub-populations of children, including those from CALD backgrounds and children with disability, who are exposed to DFV.
Structure of this report
This report begins with a review of existing literature, followed by a description of the methodology utilised. The key findings are then presented and are followed by a discussion that provides some interpretation of these findings in relation to the existing literature. The report concludes with the implications of the findings of the study for policy and practice.
State of knowledge review
A state of knowledge review was undertaken to situate the current study among the literature that focuses on children’s exposure to DFV with attention to the factors that impact their mental health.
Review methodology
This state of knowledge review was undertaken as a narrative literature review, an approach used to review and critique available evidence on a given topic or field. Narrative literature reviews are useful in providing a comprehensive overview of the topic and highlighting gaps in existing literature.
To complete this review a number of relevant databases were searched including:
- CINAHL
- Cochrane Library
- JSTOR
- Global Health via Ovid
- MEDLINE via PubMed
- SAGE
- ProQuest 5000
- PsycINFO
- Web of Science
Multiple combinations of keywords to source pertinent information were included: intimate, domestic, gender, family, violence, child, mental health, psychiatric, development, and exposure. As the literature on the outcomes of children exposed to DFV is relatively new, no year limit was set in publication searches. Research that was not published in English was excluded. The references listed in each of the sourced materials were scanned for additional relevant sources. Online searches were used to search for relevant government and non-government organisation publications and additional “grey literature”.
The final materials included in this review were original research, grey literature and unpublished reports.
The impact of DFV exposure
While many studies have investigated the impact of DFV on women, it is only in recent years that significant steps have been made to understand the impact of DFV exposure on children (Kuhlman et al., 2012), with children often referred to as “forgotten victims” (e.g. Reif & Jaffe, 2019; UNICEF, 2006).
Stress response
DFV is considered to be one of the most prevalent stressors children can experience (Margolin & Gordis, 2000), with significant evidence that environmental stressors play a major role in modifying physical and psychological health (e.g. Bair Merritt et al., 2012; Bradley & Dinan, 2010; Juruena et al., 2020). The biological mechanisms linking stress to ill-health, however, are not fully understood, but emerging literature points to a central role of the hypothalamic–pituitary–adrenal axis (HPA axis) function (Juruena et al., 2020; Margolin & Gordis, 2000). The HPA axis is an essential stress response system that enables appropriate response to stressors. While this stress response is vital to adapt to everyday stressors, chronic activation due to exposure to stressful events can challenge physiological response systems, increasing the risk for physical and psychological ill-health (Cohen et al., 2007; Juruena et al., 2020; Kiecolt-Glaser& Glaser, 2005; Mueller & Tronick, 2019).
Mental health
Existing literature has acknowledged that children exposed to DFV may experience delays in cognitive and emotional development (Antle et al., 2010; Mueller & Tronick, 2019) and an increased risk of mental illness (Carter et al., 2020; Herrenkohl et al., 2008; Huang et al., 2021; Kennedy et al., 2010; Kimball, 2016; Orr, Fisher, Preen et al., 2020). An Australian prospective pregnancy cohort study (Gartland et al., 2021) examined the mental health of children exposed to DFV and found that by 10 years of age, they were twice as likely to have anxiety as non-exposed children. Outside of Australia, a study by Olaya and colleagues (2010) captured an older range of children (8 to 17 years) attending a public mental health centre in Spain, and found that children exposed to DFV were twice as likely to have depression than non-exposed children. Similarly, Huang and colleagues’ (2021) longitudinal study of the Fragile Families and Child Well-being Study ofover 200,000 children in the United States also found higher levels of depression in children who were exposed to DFV. Their study identified DFV exposure in children under 4 years of age and followed them in five waves until the children were 15 years old. Previous longitudinal research undertaken by the authors of the current report (Orr, Fisher, Preen et al., 2020) found that Western Australian children aged 0 to 18 who were exposed to DFV before the age of 5 were three times more likely to be hospitalised during childhood for mental health disorders than non-exposed children. The mental health hospitalisations were predominately for mental and behavioural disorders due to acute stress reaction and adjustment disorders, the use of alcohol, major depressive disorder, and mental and behavioural disorders due to the use of volatile solvents.
The majority of the available literature investigating the impact of DFV on children’s mental health groups the behaviours into two distinct categories: internalising and externalising behaviours. Internalising behaviours include depression, somatic or physiological complaints, anxiety, withdrawal, suicidal ideations, eating disorders and phobias. Externalising refers to the outward expression of harmful behaviours such as aggression, hyperactivity and disobedience that affect the external environment. A meta-analysis of 60, mainly cross-sectional, studies by Evans and colleagues (2008) found an association between DFV exposure and an increased likelihood of both internalising and externalising behaviours. A more recent meta-analysis of 74 qualitative studies by Vu and colleagues (2016) also reported an increased likelihood of internalising and externalising behaviours in children exposed to DFV. However, their study went further and investigated thelong-term impact of exposure to DFV on children. They found that the association of DFV exposure and internalising and externalising problems increased over time. The authors highlight that children newly exposed to DFV may display no internalising or externalising behaviours and be thought of as being “resilient” after the exposure. However, they suggest that there may be a “sleeper effect” and the true impact on the child may not manifest for many years after the exposure.
Kernic and colleagues (2003) carried out a study with children (n=167) aged 2 to 17 in the United States whose mothers had been identified in police or court records as being subjected to DFV. They used Achenbach’s Child Behavior Checklist (Achenbach, 1991) to investigate the internalising and externalising behaviours of children exposed to DFV compared to a standardised normative sample (n=2,736) representative of the United States population. They reported that children exposed to DFV had a 60 per cent increase in risk of externalising behaviour compared to the standardised sample. However, they reported a non-significant increase for internalising behaviours compared to the standardised sample. Similarly, Campbell and colleagues’ (2013) retrospective cohort study of children with a recent child protection services investigation and DFV in the preceding 12 months found no significantly increased risk of internalising problems in the children exposedto DFV. However, they reported an 88 per cent increase in risk of externalising behaviours in children exposed to DFV six years after their recruitment in the study. The studies by Kernic et al. (2003) and Campbell et al. (2013) relied on parental reporting of children’s issues, like much of the literature investigating this area. However, the internalising problems may not be visible to the parents. A recent study (Orr et al., 2021) from the current report’s authors overcame the parental reporting issue by using linked administrative data to investigate the early development of children exposed to DFV. The study used Australian Early Development Census (AEDC) data (AEDC, 2022) which contains teacher reporting of children’s early development vulnerability. It was found that young children exposed to DFV were more likely to exhibit internalising behaviours including anxious and fearful behaviour, emotional problems and worrying compared to their non-exposed counterparts.
Olofsson and colleagues’ (2011) study (n=4,947) using data drawn from the Swedish National Health Survey reported that children (aged 0 to 18) exposed to DFV had higher odds of anxiety than non-exposed children. While the odds were significant for both male and female children, differences were apparent between the sexes: girls exposed to DFV had a six-fold increase in odds of anxiety whereas exposed boys had between a two-fold and three-fold increase, depending on their age. It has been postulated that the outcomes for girls may differ as they may be experiencing co-occurring forms of victimisation which have not been taken into account (du Plessis et al., 2015; Seng et al., 2005). These co-occurring abuses can include sexual and physical abuse (Campo, 2015). Moylan and colleagues’ (2010) prospective longitudinal study in the United States found that pre-school children exposed to DFV had higher levels of internalisingand externalising behaviours than non-exposed children. They also reported finding sex differences, with females scoring higher on internalising behaviours, and males higher on externalising behaviours. Moylan et al.’s (2010) study is not alone in finding differences between the sexes: several studies have reported that children exposed to DFV can exhibit different behavioural problems with males more likely to demonstrate externalising behaviours and females more likely to demonstrate internalising behaviours (e.g. du Plessis et al., 2015; Hosokawa & Katsura, 2019; Izaguirre & Calvete, 2018). However, Holmes and colleagues’ (2015) longitudinal study of children (n=1,125) drawn from a national survey of child and adolescent wellbeing in the United States found that among children exposed to DFV, girls were at greater risk of externalising problems than boys. Holmes and colleagues’ findings are not unique, with other researchers reporting higher rates ofexternalising in girls exposed to DFV than boys exposed to DFV (e.g. Bair-Merritt et al., 2015). Indeed, the evidence of sex is equivocal with other studies suggesting no difference or that the difference is a trend that can change with age (Sternberg et al., 2006; Vu et al., 2016).
Exposure to DFV is recognised as a precursor to post-traumatic stress disorder (PTSD) for some children (Boeckel et al., 2017; Margolin & Vickerman, 2007). The stressor criterion for PTSD in the Diagnostic and Statistical Manual of Mental Disorders (Fifth Edition; DSM-5; American Psychiatric Association, 2013) states that a person must have experienced or witnessed a traumatic event, or learned that the traumatic event occurred to a close family member. The DSM-5 stressor criterion for PTSD describes experiences commonly reported in relation to children’s exposure to DFV. Concerns have been raised (Margolin & Vickerman, 2007) that PTSD in children exposed to DFV may be misdiagnosed as another childhood condition, such as hyperactivity, depression or anxiety, due to the fact that psychological health assessments may be made without knowledge of the traumatic incident(s), namely DFV.
While PTSD is included in the DSM-5 as a diagnosable condition, growing research into the effects of trauma on child development has expanded, leading to growing calls from psychologists to include developmental trauma as a diagnostic condition (Abrams, 2021). The lack of inclusion of developmental trauma in current classifications has been argued to result in a lack of either diagnosis or assistance through mental health services. It can also result in misdiagnosis such as attention deficit disorder resulting in treatments more likely to be behavioural and medical interventions rather than trauma-focused therapies.
Burden of mental illness in children
It is estimated that one in seven Australian children aged 4 to 17 (Goodsell et al., 2017) and almost one in four Aboriginal children aged 5 to 10 (Shepherd et al., 2017) have a mental health disorder. Mental health disorders are a leading cause of disease burden in children (AIHW, 2020a). The Young Minds Matter Survey, the latest survey of child and adolescent wellbeing in Australia (Lawrence et al., 2015), reported that 43 per cent of children with a depressive disorder had severe impairment of daily living functioning. This impairment has been highlighted by Lawrence and colleagues (2019) who found that children with mental health disorders are more likely to have poor school attendance compared to their peers. Regular attendance at school is acknowledged as a crucial component of engagement in schooling and a key prerequisite for academic success (Hancock et al., 2017). Furthermore, it is accepted that mental illnessin childhood is associated with a range of poor longitudinal outcomes such as mental illness in adulthood, including mood and anxiety disorders (Nock et al., 2007; Reef et al., 2010) and substance abuse (Fergusson et al., 2007; Nock et al., 2007). Additionally, research has highlighted that mental health disorders in childhood increase the likelihood of criminal offending in adulthood (Anderson et al., 2015).
At a societal level, the economic burden of mental health disorders is substantial. Around $10.6 billion was spent on mental health services in 2018–19 (AIHW, 2021a). Child and adolescent mental health services are costly, with an average of $2,366 per patient per day (AIHW, 2021a).
Sociodemographic characteristics
Maternal mental health
It is acknowledged that women who are subjected to DFV are more likely to have mental illness than those not subjected to DFV (Karakurt et al., 2014; Langdon et al., 2014; Vilariño et al., 2018). A substantial body of evidence suggests that maternal mental illness negatively impacts children’s mental health (Barker et al., 2011; Korhonen et al., 2012; Leis et al., 2014). It is thought that maternal mental illness can impact parenting capacity (Royal Australian and New Zealand College of Psychiatrists [RANZCP], 2016; Smith, 2004); however, it has been acknowledged that the impact will vary by type of mental illness, its duration and its severity (AIHW, 2020a; Reupert et al., 2012). Maternal mental health plays a key role in children’s outcomes: in addition to the challenges surrounding parental mental illness, children exposed to parental mental illness are more likely to experience adversities compared with their non-exposed counterparts (Abel et al.,2019). It has been acknowledged that evidence-based early intervention for maternal mental illness can improve mental health outcomes for children (RANZCP, 2016).
Disability
While the effects of DFV on children’s outcomes are starting to become clearer, the effects on children with disability remain poorly understood (Dababnah et al., 2018; Robinson et al., 2020). Within Australia, 8 per cent of children under 15 years have disability (ABS, 2019). The greater dependency of children with disability on carers and family support and the time spent in the family home are thought to place the child at greater risk of DFV exposure (Baldry et al., 2006). The association between DFV exposure and intellectual disability is complex. Children exposed to DFV in utero are more likely to be born early and with a low birth weight, both of which increase the risk of intellectual disability (Bailey, 2010; Dababnah et al., 2018). Additionally, being subjected to DFV in pregnancy has been correlated with congenital malformations (Hansen et al., 2000; Orr et al., 2022; Ortega-García et al., 2013). Exposure to DFV in utero has also beenassociated with lower IQ scores in children (Huth-Bocks et al., 2001; Koenen et al., 2003; Ybarra et al., 2007), poorer cognitive ability (Orr et al., 2021; Udo et al., 2016) and developmental delays (Dababnah et al., 2018; Udo et al., 2016).
Culturally and linguistically diverse status
Australia has a long history of migration (Collins, 2013). The most recent Australian Census (ABS, 2021a) reported that 62 per cent of Western Australians have one or both parents born overseas. The evidence as to whether prevalence of DFV is higher or lower in CALD women compared to Australian-born women is equivocal (Cox, 2015; Ghafournia & Easteal, 2018). CALD women’s experiences of DFV are often exacerbated through the intersectional nature of forms of oppression, such as racism; changed and changing gender and family roles (Fisher, 2013); and social factors including social isolation (Carline & Easteal, 2014) and lack of awareness of available services (Ghafournia & Easteal, 2018).
Concurrently, evidence is lacking on the outcomes of children who are exposed to DFV and born to CALD parents. This may be due to those from CALD backgrounds not being identified in samples or underrepresented within research.
The most recent Young Minds Matter Survey (Lawrence et al., 2015) in Australia reported mental illness to be less common in children with both carers born overseas (5%) than those with both carers born in Australia (14%). However, findings in this area are equivocal with Minas and colleagues (2013) reporting similar levels of mental illness in children of migrant parents and children of Australian-born parents.
Child maltreatment
Children exposed to DFV are at increased risk for child maltreatment (Herrenkhol et al., 2008; Orr, Fisher et al., 2019), with a concomitant three-fold increased risk of poorer mental health outcomes than their non-abused peers (Maclean et al., 2019). Child maltreatment is generally considered to be behaviour towards a child which has a risk of causing physical or emotional harm from physical abuse, sexual abuse, emotional abuse and/or neglect (Australian Institute of Family Studies [AIFS], 2018), with maltreatment significantly contributing to child mortality and morbidity (Chen et al., 2016; Gilbert et al., 2009; Segal et al., 2021). Chronic stress from the trauma is thought to impact the child’s brain which can result in health problems (National Scientific Council on the Developing Child, 2012). In recent years children’s exposure to DFV has been acknowledged as a type of maltreatment (AIFS, 2018; Graham-Bermann, 2011; Richards, 2011).However, differences exist between state and federal definitions within Australia. The Commonwealth Family Law Act 1975 recognises that exposure to DFV is a form of child abuse – specifically, psychological harm. The Act defines exposure as occurring “if the child sees or hears family violence or otherwise experiences the effects of family violence” (pt I, s 4AB). The Western Australian Children and Community Services Act 2004 widened its definition of emotional abuse, in 2016, to include children’s exposure to DFV. They use the definition from the Restraining Orders Act 1997 (WA). Exposure in this context is defined by the child seeing or hearing the DFV or witnessing physical injuries resulting from DFV. Historically, mothers subjected to DFV have been blamed for not maintaining the safety of their children. However, this is rightfully changing with a growing focus on perpetratoraccountability including the development of policies and practice in child protection on how to respond to DFV (e.g. Government of Western Australia, 2015).
While it is widely cited that there is a considerable overlap between DFV and other types of child maltreatment (e.g. Gracia et al., 2018; Herrenkohl et al., 2008), the extent of this overlap varies significantly in the literature. This may be due in part to robust estimates of any association being difficult to confirm due to the variability in the definitions of child maltreatment, DFV and exposure within the literature. That being said, from a review of 10 studies presenting prevalence of the co-occurrence of DFV with other forms of child maltreatment, Bidarra and colleagues (2016) estimated the prevalence to be between 12 per cent and 70 per cent. Previous research (Orr, Fisher et al., 2019) on Western Australian children (n=524,534) born in a 20-year period found that 41 per cent of children whose mothers were hospitalised for DFV were known to child protection services. Given the high level of overlap among types of maltreatment and links tomultiple poor outcomes (e.g. Maclean, Taylor et al., 2017; Mills et al., 2012) it is difficult to isolate to the effect of a single maltreatment type on a specific outcome.
Socioeconomic status
Despite DFV occurring across all economic strata, low socioeconomic status (SES) has been acknowledged as a risk factor for women subjected to DFV (Orr, Preen et al., 2019; Orr, Fisher, Preen et al., 2020; Reichel, 2017). Low SES is also associated with mental health disorders in childhood, with the most recent national survey of Australian children and young people reporting higher prevalence of mental health disorders in children from low SES than in those residing in higher SES areas (Lawrence et al., 2015).
Aboriginal and Torres Strait Islander children
Based on data from the 2014–15 National Aboriginal and Torres Strait Islander Social Survey (ABS, 2016b), Aboriginal and Torres Strait Islander women experience high rates of DFV. As a result, Aboriginal and Torres Strait Islander children may be more likely to live in homes where violence is present than non-Aboriginal and Torres Strait Islander children. The National Plan to Reduce Violence against Women and their Children 2010–2022 (Council of Australian Governments, 2011) acknowledges the disproportionate rates of DFV and children’s exposure to it as a national priority.
Research indicates that Aboriginal and Torres Strait Islander children are more likely to have poorer mental health than their non-Aboriginal and Torres Strait Islander peers (AIHW, 2018c; Al-Yaman, 2017). The disparity in mental health is the result of cultural genocide, colonisation and racism (Calma et al., 2017; Marmot, 2011; Shepherd et al., 2017). The mental health of Aboriginal and Torres Strait Islander children is a priority in the national agreement between the Australian Government and the Coalition of Aboriginal and Torres Strait Islander Peak Organisations in their commitment to “close the gap” (Commonwealth of Australia. Department of the Prime Minister and Cabinet, 2021) between the outcomes for Aboriginal and Torres Strait Islander and non-Aboriginal and Torres Strait Islander children. Research specific to Aboriginal and Torres Strait Islander children’s experiences of DFV and mental illness is lacking, and it is an area in need ofinvestigation.
Resilience
It is important to note that not all children exposed to DFV will have negative outcomes. Some children who experience adverse events in childhood adapt well and show no maladjustment in their psychological development (Masten, 2001). Children who do not develop negative outcomes and adapt successfully when exposed to adverse circumstances are considered resilient (Howell, 2011). Resilience is a dynamic construct, changing in response to external and internal events and conditions (Herrman et al., 2011; Masten, 2011). It has been described as an individual’s adaptation to manage or cope with significant adversity, risk or stress, which may result in an increased capacity to respond to future adversity (Herrman et al., 2011; Lemerle & Stewart, 2011; Luthar et al., 2000). It is widely accepted that resilience is not only derived from individual personal characteristics but also from external circumstances such as social and cultural determinants(Cicchetti & Valentino, 2006; Study of Environment on Aboriginal Resilience and Child Health Investigators, 2010). The socio-ecological model (Bronfenbrenner, 1977) has been used in this report to identify factors across internal and external systems that influence resilience (Henderson et al., 2016; Howell, 2011). However, as highlighted earlier in this section there may be a “sleeper effect” and the true impact on the child may not manifest for many years after the exposure (Vu et al., 2016).
Using linked administrative data for research on children exposed to DFV
Much use has already been made of the large linked administrative databases in Western Australia to investigate outcomes of children’s adverse childhood experiences, including maltreatment and incarcerated parents (e.g. Bell et al., 2018; Hafekost et al., 2017; Maclean et al., 2020). However, the use of linked administrative data to investigate the impact of DFV on children is emerging. Linked administrative datasets provide numerous research benefits. Firstly, such data are based on the whole population which reduces selection biases that are present in most DFV exposure research, such as small samples drawn from refuges and other specialist services. Specialist services are often used for sampling for a plethora of reasons including difficulty in identifying children exposed to DFV, maintaining the safety of the child and their family, and ensuring that the children have appropriate mental health support when recalling their experiences (Btoush &Campbell, 2003; Fraga, 2016; Paavilainen et al., 2014). Utilising linked administrative data overcomes many of these issues. Furthermore, we are able to investigate important groups such as Aboriginal and Torres Strait Islander children and children with disability utilising administrative data because, as noted, it includes the whole population. Linked administrative data also provides access to important factors that can impact on the outcomes of children and be adjusted for in analysis, such as SES, mother’s marital status and mother’s mental health.
Conclusion
Exposure to DFV is a significant stressor for Australian children. Existing literature highlights that exposure to DFV is associated with poorer mental health in childhood. However, the literature is limited by the predominant use of cross-sectional studies with little account given to the mental health impacts that may occur over time. Existing research has also focused on the grouping of mental health issues into internalising and externalising behaviours which can restrict targeted interventions. Additionally, there is a need to conduct research in an Australian context given the disparity of both exposure to DFV and mental illness for Aboriginal and Torres Strait Islander children. Children exposed to DFV may not present with mental illness for many years. The use of longitudinal linked administrative data provides a clearer understanding of the long-term impact of DFV exposure on children’s mental health and takes into account factors that arelikely to co-occur with DFV exposure that will also impact their mental health. The lack of available evidence to inform best-practice principles for interventions for children exposed to DFV means that current interventions may be sub-optimal, or even inappropriate. This project provides an opportunity to identify areas for targeted and evidence-based interventions and polices by utilising the best possible data.
Methods
The objective of this study was to explore the mental health service use of, and mental health diagnosis associated with, children exposed to DFV. This was achieved via a population-based cohort study using de-identified linked administrative data of children born in Western Australia between 1987 and 2010. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting checklist (von Elm et al., 2008) was used to guide this report.
Conceptual framework
In acknowledgement of the disproportionate levels of violence against women perpetrated by men this study was underpinned by feminist theory (Dobash & Dobash, 1979; Yodanis, 2004). Additionally, a socio-ecological model (see for example Heise, 1998) was adopted as the conceptual framework for this study. Ecological models were introduced in the 1970s by Bronfenbrenner (1977) to explain how the interactive environment affects a child’s growth and development. It was argued that human development is the product of bi-directional interactions (processes) between an individual (person) and the many developmental settings (context) to which the individual is exposed over the life course (time; Bronfenbrenner, 1994). The socio-ecological model has also been used to integrate the array of personal, situational and social factors that interact to gain understandings of DFV (Heise, 1998), with the WHO adopting Heise’s ecological model in their work onDFV (WHO, 2020b). The model is appropriate for the current study as children exposed to DFV are more likely to live with multiple stressors (McGavock & Spratt, 2017) and an ecological framework is a useful approach to consider the complex variables that influence a child’s mental health (D’Andrea & Graham-Bermann, 2017). The model is also able to incorporate both feminist and social science insights.
Data sources
An overview of the data collections and the main variables extracted for the research presented in this report are shown in Table 2.
Table 2: Data collection variables and periods of coverage used in this report
Dataset
Period of coverage contained in this report
Main variables extracted
WA Registry of Births, Deaths and Marriages
1987–2010
Date of birth (mm/yyyy)
Sex
Gestation
Born in hospital
Mother’s age
Birth weight
Midwives Notification System
1987–2010
Date of birth (mm/yyyy)
Sex
Maternal age
Maternal marital status
Mother’s previous pregnancies
Gestation
ARIA a
SEIFA b
Hospital Morbidity Data Collection (HMDC)
1970–2016
Admission date
Separation date
Age at admission
Principal diagnosis
External cause codes
Additional diagnosis
Emergency Department Data Collection (EDDC)
2002–2016
Presentation date (mm/yyyy)
Principal diagnosis
External cause of injury code
Mental Health Information System (MHIS)
1970–2017
Primary diagnosis
Date of birth (mm/yyyy)
Age at contact
Episode start date
Date of contact
Department of Communities, Child Protection and Family Support (CPFS) dataset
1990–2016
Reason type
Reason start date
Reason end date
Primary nature of concern
Period of care start date
Period of care end date
Western Australian Register of Developmental Anomalies (WARDA)
1987–2016
Diagnosis code
Major or minor malformation
Sex
Intellectual Disability Exploring Answers (IDEA) dataset
1987–2016
Level of intellectual disability
Date of birth (mm/yyyy)
Type of disability
Western Australia Police Force Incident Management System (IMS)
2004–2008
Offence
Partner type
Children present
Location of offence
Notes: a.Accessibility/Remoteness Index of Australia.
b Socioeconomic Indexes for Areas.
Mental Health Information System
The MHIS has been collecting information since 1966 and includes all records of patients using inpatient and outpatient public mental health services and private inpatient services. Inpatient data are collected from mental health hospital wards and community accommodation support programs. Outpatient information is collected from psychiatric clinics, triage services, community mental health centres, psychiatric day centres and rehabilitation programs. Clinical data that are collected include principal diagnosis, start and end date of the mental illness episode, and the date that the individual utilised mental health services. The diagnosis is coded using ICD codes. The MHIS data also includes demographic details (e.g. age, sex).
Hospital Morbidity Data Collection
The HMDC is a database of information about hospital admissions. It includes summaries of all admission records for both public and private hospital inpatients. Records are structured on a patient’s episode of care, with each record containing information regarding an admission and clinical procedures carried out, discharge and separation from hospital, and demographic information. The diagnosis information includes one principal diagnosis, up to four co-diagnoses, and up to 20 additional diagnoses. The record also contains external cause of injury codes. This information can include place of event and circumstances of the injury. The HMDC has been in operation since 1970 and in that time it has utilised several editions of ICD codes. The ICD-8 was utilised between 1970 and December 1978; the ICD-9 was used between January 1979 and December 1987; the ICD-9-Clinical Modification (ICD-9-CM) was used between January 1988 and June 1999; and theICD-10-Australian Modification (ICD-10-AM) has been used from July 1999 until the present date.
Emergency Department Data Collection
The EDDC includes information on all presentations to emergency departments of public hospitals in Western Australia, as well as emergency department activity in private hospitals under contract with the Western Australian Government. Records in this collection date back to 2002. Information recorded includes primary diagnosis (when applicable), coded per ICD-10-AM, and demographic information including date of birth, sex, Aboriginal and Torres Strait Islander status and country of birth.
Cohort selection
Exposure to DFV was initially identified in children born between 1987 and 2010 (inclusive) whose mother was identified in Western Australia Police Force IMS data from 2004 to the end of 2008 as a victim of DFV where a male perpetrator was charged for the offence and a domestic relationship indicator was recorded. This approach has been used in previous research (Orr, Fisher, Preen et al., 2020; Orr, Fisher, Glauert et al., 2020). The criminal offences included were murder, attempted murder, assault and injury, sexual assault, threatening behaviour and misuse of weapons/explosives. There were 15,598 children born to mothers who were identified as victims of DFV in police data during the period 2004 to 2008 (inclusive). Children were initially individually matched at a ratio of 1:3 (15,598:46,438) to a non-DFV (i.e. non-exposed) cohort of children based on month of birth, SES, Aboriginal and Torres Strait Islander status and sex. Due to the hiddennature of DFV (Francis et al., 2017) we also examined non-exposed children for any maternal DFV hospitalisations by interrogating the hospital records of their mothers from 1979 to 2016 (inclusive) using ICD codes used in previous research (Orr, Preen et al., 2019; Orr, Fisher, Preen et al., 2020). We found that 4,442 originally “non-exposed” children had a mother who was hospitalised for DFV-related injuries. Finally, we identified children in the exposed group who were exposed to DFV between birth and 18 years. This resulted in an exposed cohort of 16,356 and a non-exposed cohort of 41,996 children (Figure 1).
Figure 1: Cohort selection flowchart
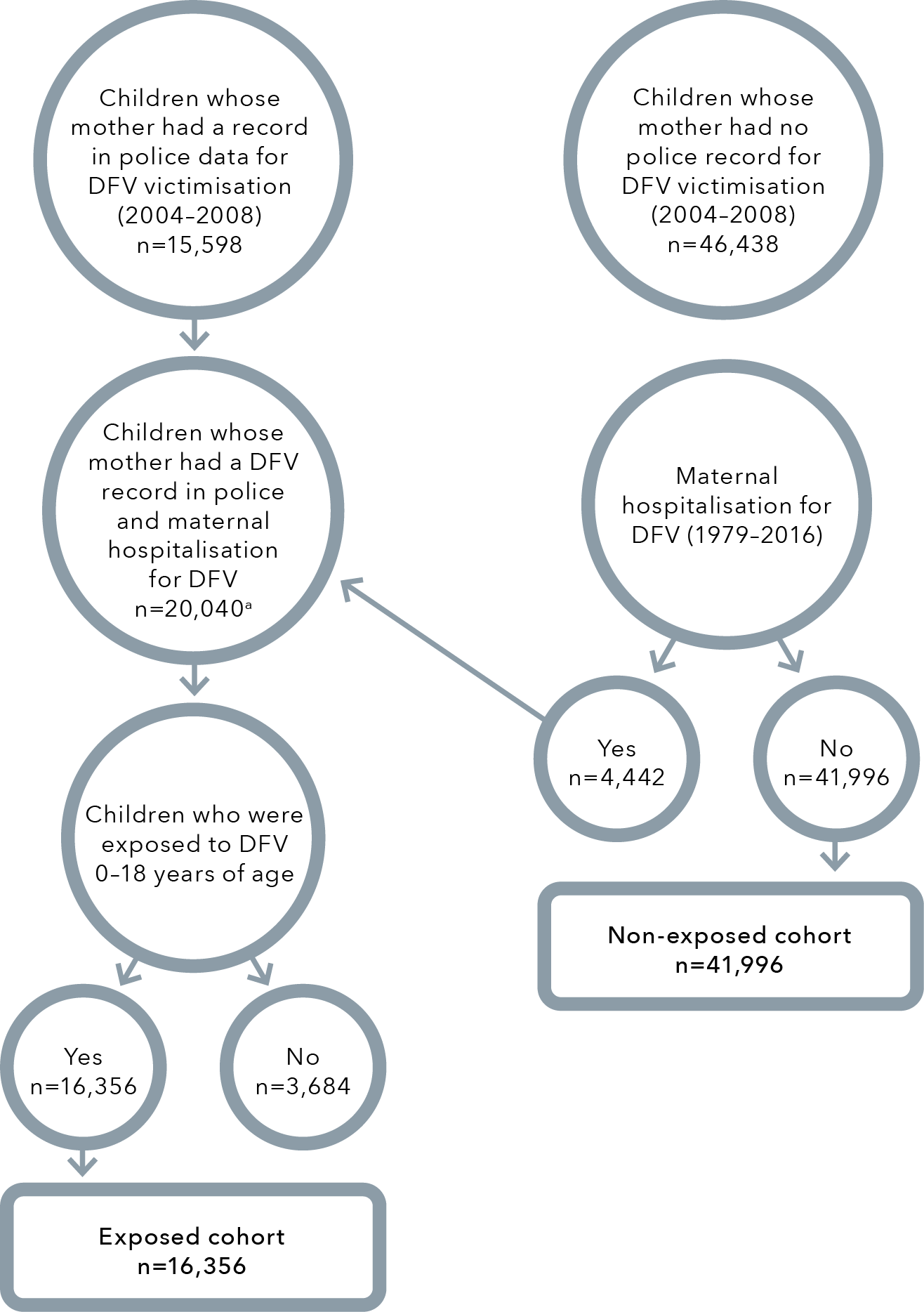
Note: a Includes the 4,442 children identified in the original cohort of children whose mother had no police record for DFV victimisation (2004–2008) but had a maternal hospitalisation for DFV.
Data linkage
Data linkage is defined as “the bringing together[,] from two or more different sources, data that relate to the same individual, family, place or event” (Holman et al., 2008, p. 767). Data linkage involves the linkage of administrative (and other) data that are collected by governments and non-government agencies for service delivery and administrative purposes. These data are commonly collected at the population level, can be made available for research and contain rich, detailed information. The linking of data sets from multiple sources can provide greater insights than those generated by single sources (Harron et al., 2017). While population-level administrative data do not capture the level of detail that may be sourced from survey data, linked individual-level administrative data has become an attractive alternative as it provides longitudinal information; is free of biases which typically affect survey data such as recall, response andselection biases, and attrition; and it is comparatively cost-effective as the data are already collected (Jutte et al., 2011; Pearson, 2015). Linked administrative data can provide large sample sizes and detailed data on hard-to-reach populations, such as children exposed to DFV, enabling evidence to be generated with a high level of external validity and applicability for policymaking (Harron et al., 2017).
Data custodians are the gatekeepers of administrative datasets and have a number of rights and responsibilities in relation to the release and access of datasets by researchers (Australian Government, 2018), including ensuring that the research project is of public benefit.
Datasets were linked, for both exposed and non-exposed groups, by the Western Australian Data Linkage Branch using probabilistic linkage (Holman et al., 1999). Data were provided as individual linkable datasets to the report authors, then de-identified and merged using a project-specific encrypted linkage key (Kelman et al., 2002). No identifiable information was received by the researchers involved in this study.
The Western Australia Police Force provided data from their IMS to the Western Australian Data Linkage Branch for women who had been subjected to DFV that resulted in the male perpetrator being charged with an offence. The children of the females subjected to DFV were linked by the Data Linkage Branch using the WA Midwives Notification System.
WA Family Connections System
The WA Family Connections System contains links between individuals who are related, created using information from datasets that identify multiple related people, for example Birth Registrations and Midwives’ Notifications (Glasson et al., 2008). These relationships are usually biological. No information is known about adoptions, including step, local or overseas adoptions; other care arrangements; or divorces. The genealogy held by the Data Linkage Branch includes parents and siblings of people born in Western Australia since 1945. Extended family members (including grandparents, grandchildren, cousins, aunts and uncles) can also be identified (Government of Western Australia Department of Health, 2022). Links are available for people born in Western Australia and their family members who have migrated to Western Australia and had contact with one of the government agencies listed in Table 2. To connect the family members the researchers wereprovided with a separate mapping file that include a “linkage key” for the child matched to a corresponding linkage key for the family member. For this study linkage keys were provided to connect a child with their mother and their father across datasets.
Consent
Administrative data in Western Australia are collected without consent. To ensure confidentiality and ethical practice, strict processes exist for access to linked administrative data. To gain access to data, researchers must adhere to the Data Linkage Branch’s Access and Charging Policy. Researchers are required to discuss potential projects with the data custodian of each database from which they are requesting data and gain their approval to access the data. Aboriginal data sovereignty
affirms the rights of Indigenous peoples to determine the means of collection, access, analysis, interpretation, management, dissemination and re-use of data pertaining to the Indigenous peoples from whom it has been derived, or to whom it relates. (Walter et al., 2021, p. 4)
This project engaged with Aboriginal people and Aboriginal community-controlled organisations (see “Community and consumer involvement” subsection for further detail) about the design and interpretation of the data. Additionally, approval was gained from the Western Australian Aboriginal Health Ethics Committee (WAAHEC), with WAAHEC reviewing the report prior to publication. WAAHEC monitors outputs to ensure that they are ethically sound and culturally appropriate, as well as to ensure benefit to Aboriginal and Torres Strait Islander peoples.
Cohort characteristics
Domestic and family violence exposure
Western Australia Police Force data have a mandatory “domestic flag” variable which has been recorded since the implementation of the Frontline IMS system in 2004. This variable draws on the type of behaviour alleged and the relationship between the parties.
The type of DFV is indicated in police data by the Australian and New Zealand Standard Offence Classification (ABS, 2011a) subdivision level. The DFV types are murder and attempted murder, assault and injury, sexual assault, threatening behaviour, and misuse of weapons/explosives (see Appendix A for further details). The data from IMS made available to the researchers were from 1 January 2004 to 31 December 2008.
HMDC records do not contain a “DFV flag”. Therefore, records of the mothers were searched for ICD codes used in previous studies (Orr, Preen et al., 2019; Orr, Fisher, Preen et al., 2020) that identify DFV (Table 3).
The project is based on the assumption that children in the majority reside with their mother as primary caregiver.
Table 3: ICD codes identifying DFV
ICD code
Definition
ICD edition
E960–E969
Homicide and injury purposely inflicted by other persons
ICD-9 a
995.81
Adult physical abuse
ICD-9 a
V71.5
Observation following alleged rape or seduction
ICD-9 a
E980–E989
Injury undetermined whether accidentally or purposely inflicted
ICD-9 a
V61.1
Counselling for marital and partner problems
ICD-9 a
T74.1
Physical abuse
ICD-10-AM b
T74.2
Sexual abuse
ICD-10-AM b
T74.3
Psychological abuse
ICD-10-AM b
Z04.4
Examination and observation following alleged rape or seduction
Examination of victim or culprit following alleged rape or seduction
ICD-10-AM b
X85-Y09
Assault
ICD-10-AM b
Y10-Y34
Event of undetermined intent
ICD-10-AM b
Z63.0
Problems in relationship with spouse or partner. Discord between partners resulting in severe or prolonged loss of control, in generalisation of hostile or critical feelings or in a persisting atmosphere of severe interpersonal violence (hitting or striking)
ICD-10-AM b
Notes: a International Classification of Diseases Ninth Edition.
b International Classifications of Disease 10th Edition Australian Modification.
Aboriginal and Torres Strait Islander status
Aboriginal and Torres Strait Islander children were identified by the Western Australian Data Linkage Branch derived Aboriginal status flag. The flag, developed by the Data Linkage Branch in collaboration with the Australian Institute of Health and Welfare (AIHW), is derived by a validated algorithm when an individual is recorded as Aboriginal and/or Torres Strait Islander in Western Australian Government administrative data sets (Christensen et al., 2014).
Disability
Disability was flagged from three sources: first, a record of the child in WARDA datasets as having a birth defect or cerebral palsy, and second, intellectual disability captured in the IDEA database. Third, following consultation with advisors from WARDA, ICD codes were identified (Table 4) that were used to search the child’s HMDC records to further capture disability.
Table 4: ICD codes capturing disability
Disability description
ICD-9
ICD-10
Intellectual disability
317–319
F70–F79
Autism
299.0
F84.0, F84.1
Down syndrome
758.0
Q90
Cerebral palsy
343
G80
Birth defects
740–759 (excluding 758.0)
243, 246.1, 255.2, 270, 271.3, 272.4, 271.0, 271.1, 271.2, 272.3, 271.8, 272.7, 330.1, 277.5, 271.8, 271.9, 272.7, 277.2, 277.1, 277.4, 277.8, 275.1, 275.3, 275.4, 277, 272.6, 277.6, 277.8, 330.2, 330.4, 330.8, 331.9, 359.0, 359.1, 359.2
Q00–Q99 (excluding Q90)
E03.0, E03.1, E25.0, E25.9, E70–E73.0, E74.0–E74,4, E75, E76, E77, E79.1, E79.8, E79.9, E80.0-E80.5, E83.0, E83.3, E83.5, E84, E88.0, E88.1, E88.8, G31.8, G31.9, G32.8, G71
Culturally and linguistically diverse children
We aimed to investigate the mental health service contact and mental health diagnosis by subtypes of CALD children who were exposed to DFV compared with non-CALD children exposed to DFV. However, this was unable to be empirically examined due to limitations in the data.
Socioeconomic status
Neighbourhood-level SES was determined by the Socio-Economic Indexes for Areas (SEIFA) using the Midwives Notification System. The SEIFA score is based on information from the Australian Census about income, education, employment, occupation and housing, and provides a measure of relative SES for the area where a person resides. Five levels of disadvantage were assigned to Census collection districts (~250 households), ranging from 1 (high disadvantage) to 5 (low disadvantage; ABS, 2018a).
Residential remoteness
Residential remoteness was determined by the Accessibility/Remoteness Index of Australia (ARIA), based on the distance of geographic locations from the nearest population centre, ranging from major cities to very remote Australia (ABS, 2018b). Residential remoteness was identified in the Midwives Notification System from collection district, with the smallest spatial unit available equating to approximately 250 households (ABS, 2011b).
Mothers’ mental health service contact
Mothers’ mental health service contact was identified if the mother had a record in the MHIS dataset, which included both public and private inpatient services and public outpatient services for psychiatric care. HMDC records were also searched for mental health admissions. Mothers’ mental health contacts occurring after a child’s first mental health contact were excluded from analysis.
Maternal marital status
Mothers’ marital status was identified in the Midwives Notification System. They were grouped into four categories: married/de facto/widowed, never married, divorced/separated and unknown/not stated.
Parents’ age
Mothers’ age at the child’s birth was identified in the Midwives Notification System and grouped into four categories: under 20 years, 20–29 years, 30–39 years and 40 years and over. Fathers’ age details were also identified in the Midwives Notification System and groups using the same categories as above. Not all children had their father’s age available so a fifth category of “missing age” was added.
Early gestation
Early gestation was identified in the Midwives Notification System. A child born prior to 37 weeks gestation was classified as being born pre-term.
Child protection involvement
Child protection involvement was identified in the Western Australia Department of Communities dataset where a notification had been made regarding concern for the child. A child was deemed to have been in contact with child protection services if they had ever had at least one record of notification, period of care, order, placement or application within the child protection and family support data sets. Child protection involvement was moderately correlated with DFV (> 0.6), which can make it difficult to separate the effects of each risk factor. Using variance inflation factors (VIF) to test for collinearity, child protection involvement and DFV had VIF=1.82, meaning no evidence of collinearity. However, as DFV is a recognised form of child abuse (Richards, 2011), child protection was excluded in analysis due to the conceptual similarities and the challenge of disentangling the effect (Richards, 2011).
Outcomes
The primary study outcomes were childhood mental health service contact and mental illness diagnosis. Children were followed from birth until end of follow-up on 31 December 2017, date of death or the age of 18, whichever came first. Outcomes were examined in the cohort overall and separately in Aboriginal and Torres Strait Islander children and children with disability.
Mental health service use was ascertained by combining records of mental health contacts/discharges and diagnoses across the HMDC, MHIS and EDDC data collections. The primary diagnosis code in HMDC is mandatory; HMDC records used in this study had fully populated primary diagnosis. Population of diagnosis in EDDC is not mandatory, and 68.5 per cent of EDDC records used in this study had principal diagnosis missing. MHIS data had 39.7 per cent of records missing a primary diagnosis. The overall measure of mental health service contact was defined as a child having had any mental illness-related diagnosis (yes/no) in HMDC or EDDC data and/or any recorded contact in MHIS during the follow-up period. Only a child’s first mental illness-related contact after DFV (across the three data collections) was considered for modelling purposes relating to overall service contact.
Mental health diagnosis was captured by utilising ICD codes to identify diagnostic outcomes. These diagnoses were grouped according to mental health types. Mental health diagnoses were categorised into 10 main groupings (Table 5). Self-harm was included in mental health service contact and diagnosis grouping: while self-harm is not a mental illness it is often linked to mental distress. The inclusion of self-harm in mental health service contact is an approach used in previous research (Maclean et al., 2019). It is important to note that children with more than one diagnosis during childhood could be counted in multiple diagnostic groups.
Table 5: Mental illness-related ICD diagnostic codes
Mental illness group a
ICD-9 codes
ICD-10 codes
Organic disorder
290, 293, 294
F00–F09
Substance use disorder
292, 304, 305
F10–F19, F55
Schizophrenia and psychoses
295, 297, 298
F20–F29, F30, F31, F32, F33, F34.8, F34.9, F38, F39
Depressive disorder
296, 300.4, 311
F32.0, F32.9, F33.0, F34.1
Anxiety disorder
300, 300.0, 300.2, 300.3, 300.8, 308, 309
F40–F45, F48, F63.3, F68
Personality disorder
301
F60, F61, F62, F68, F69
Psychological development disorder
299, 307.2, 307.3, 307.6, 307.7 312, 313, 314, 315
F80–F89, F90–F98
Intentional self-harm
E950–E959
X60–X84
Other mental illness-related contacts
300.1, 300.5, 300.6, 300.7, 300.9, 302, 306, 307.0, 307.1, 307.4, 307.5, 307.8, 307.9, 310, 316
F44, F50–F54, F59, F64, F65, F66, F99
Mental health contact with no diagnosis recorded b
No mental illness-related ICD codes
No mental illness-related ICD codes
Notes: a Children with more than one diagnosis could be counted in multiple diagnostic groups.
b Comprises children with a mental health contact in MHIS who had no mental health diagnosis and had no other mental health diagnosis identified in HMDC or EDDC data.
Community and consumer involvement
Community and consumer consultation
Prior to the initiation of the project, members of the research team undertook a research priority setting process through a partnership with those with lived experience of DFV, their informal support people and DFV service providers. This priority setting process highlighted that the impact of DFV on children was a priority area for research (Fisher et al., 2016). The researchers also met with the Developmental Pathway Project Community and Consumer Group at the Telethon Kids Institute to gain feedback and comment on the proposed research. Meetings were also held with the Kulunga Aboriginal Research Development Unit (KARDU) at the Telethon Kids Institute, which is involved with building the capacity and development of researchers working on research projects that include a focus on Aboriginal outcomes. Meetings were also held with Ruah Community Services, an organisation providing community DFV services. Additionally, discussions were held with seniorstaff at Aboriginal community-controlled health services within Western Australia. Support for the research was gained from the Wirraka Maya Health Service Aboriginal Corporation and Moorditj Koort Aboriginal Health and Wellness Centre.
Post-initiation project support was provided by the Wungening Aboriginal Corporation to help facilitate a reference group to discuss and interpret report findings prior to publication.
Reference group
In addition to the community and consumer involvement outlined above, this project included three reference groups, the members of which provided feedback and advice on the interpretation of the research results and the implications of key findings for policy and practice. The first reference group was recruited by the WA Health Translation Network and comprised both Aboriginal and non-Aboriginal women with lived experience of DFV and/or mental illness. The second reference group comprised Aboriginal and Torres Strait Islander women with lived experience of DFV who were residing in a refuge service provided by Wungening Aboriginal Corporation. The third reference group was the Linking for Life community and consumer group, members of which have an understanding of using linked administrative data for research.
Statistical analysis
Descriptive analysis was conducted for all variables. Sociodemographic variable groupings were initially assessed for crude associations using Chi-square tests. Multivariate Cox regression was used to estimate the association between DFV and mental health service contact in children, with separate analyses for mental health sub-type groupings and by Aboriginal and Torres Strait Islander status and children with disability. Estimates are presented as adjusted and unadjusted hazard ratios (HR) with Wald 95 per cent confidence intervals (CI). Kaplan-Meier survivor function estimates for all categorical covariates were approximately parallel and hence each adhered to the proportional hazards assumption (Kleinbaum & Klein, 2012). Collinearity of covariates was tested using variance inflation factors where VIF>10 was deemed to be collinear (Vittinghoff et al., 2012). No covariates considered for modelling were collinear based onthese conditions. Models were adjusted for known sociodemographic confounders including sex, Aboriginal and Torres Strait Islander status, gestational period, SEIFA and ARIA. Parental sociodemographic factors were also included in the models as potential predictive variables, such as mother’s age at birth, father’s age at birth, marital status and previous mental health service contact by the mother. Potential predictors known to increase the risk of the outcome were included. Each potential predictor was analysed separately to determine the univariate association with the outcome variable. Results in which the 95 per cent CIs did not include the null value of 1 were considered statistically significant. Time to first mental health-related contact was measured in months from birth. All models were tested for interactions, with no combinations showing significance at the p<0.05 level.
A random assignment of virtual DFV exposure was applied to children not exposed to DFV matched by birth year to account for different cohort follow-up periods in children exposed to DFV and those not exposed. Non-exposed children assigned virtual times to mental health service contact that exceeded their total length of available follow-up were excluded from analysis (n=815).
The predicted number of mental health contacts was calculated to plot the trajectories of children exposed and not exposed to DFV according to different sociodemographic characteristics. Trajectories demonstrated time (in months) from first DFV (“time zero”) until first mental health service contact (or censored at death or once they had reached 18 years of age). All analyses were performed using Statistical Analysis System (SAS) statistical software (version 9.4) using the PHREG and LIFETEST procedures.
To investigate mental health service use over time we used trajectory plots to show the estimated cumulative probability (i.e. chance) of a child experiencing a mental health service contact over time (in years) from their birth until they reached 18 years of age. The trajectories are categorised according to those who had been exposed to DFV and those who were not exposed. These subgroups were further categorised according to a series of sociodemographic characteristics that are associated with higher risk of mental health contacts – specifically sex, SES, disability status and Aboriginal and Torres Strait Islander status. Cumulative probability curves were compared for differences using Gray’s test (Gray, 1988). A Gray’s p-value<0.05 was considered a statistically significant difference.
To identify key sociodemographic characteristics of mental health diagnosis and diagnosis subtypes of children with known DFV we stratified our analysis by DFV exposure. Findings for non-exposed children allow comparison.
Research indicates that Aboriginal and Torres Strait Islander children are at an increased risk of exposure to DFV (ABS, 2016b) and mental illness compared to non-Aboriginal and Torres Strait Islander Australians (AIHW, 2018c). To gain an insight into the characteristics that increase the risk of mental health service contact for Aboriginal and Torres Strait Islander children we stratified our analysis by exposure to DFV. We also examined the risk of having a mental health diagnosis subtype for Aboriginal and Torres Strait Islander children exposed to DFV and Aboriginal and Torres Strait Islander children not exposed to DFV.
To gain an insight into the impact exposure to DFV has on Aboriginal and Torres Strait Islander children we examined the subcategories of mental health of exposed Aboriginal and Torres Strait Islander children compared to non-exposed Aboriginal and Torres Strait Islander children. We also investigated the subcategories of mental health for non-Aboriginal and Torres Strait Islander children exposed to DFV compared to non-exposed, non-Aboriginal and Torres Strait Islander children.
It is acknowledged that children with disability are more likely to have mental illness than children without disability (Emerson & Hatton, 2007; Hebron & Humphrey, 2014; Wadman et al., 2011). To gain an insight into the characteristics that increase the risk of mental health service contact for children with disability we stratified our analysis by disability status. We also examined the subcategories of mental health diagnosis of children with disability exposed to DFV compared to non-exposed children with disability.
Ethics
Ethics approval was gained from the Western Australian Department of Health Human Research Ethics Committee (#2016.60), the Western Australian Aboriginal Health Ethics Committee (#756) and The University of Western Australia Human Research Ethics Committee (RA/4/1/8867).
Results
Cohort sociodemographic characteristics
There were 58,352 children in our cohort, comprising 16,356 (28%) children who were exposed to DFV between birth and 18 years of age, and a non-DFV-exposed comparison group of 41,996 (72%) matched children. Table 6 highlights the characteristics of the children in the cohort.
Aboriginal and Torres Strait Islander children were over-represented in our cohort when compared to the state of Western Australia. According to the 2016 Census (ABS, 2018c), only 7 per cent of people under 18 years in Western Australia were Aboriginal and Torres Strait Islander, compared to 62 per cent of children in our exposed group and 50 per cent in our non-exposed group.
The exposed group also had a higher proportion of being born to teenage mothers (26% versus 15%) and unmarried mothers (31% versus 19%) and having a mother with a mental health disorder (45% versus 21%), compared to the non-exposed children. A higher proportion of children exposed to DFV were from a very remote area (21%) compared to non-exposed children (13%).
Over half of the children exposed to DFV were known to child protection services (53%). This proportion is considerably higher than the 4 per cent seen in the non-exposed group and higher than the national rate of 3 per cent reported by the AIHW (2021b).
A higher proportion of the exposed cohort had a mental health service contact compared to the non-exposed cohort (23% versus 11%).
There was a significant difference (p<0.0001) between the average age of mental health contact for children exposed to DFV (12.5 years) compared to non-exposed children (11.6 years). The average age of DFV exposure in our exposed group was 6.5 years.
Table 6: Sociodemographic information of the cohort
Aboriginal and/or Torres Strait Islander
Characteristic
Childhood DFV
N (%)
No recorded childhood DFV
N (%)
p-value c
Yes
10,205 (62.4)
20,919 (49.8)
<0.0001
No
6,151 (37.6)
21,077 (50.2)
Sex
Characteristic
Childhood DFV
N (%)
No recorded childhood DFV
N (%)
p-value c
Female
7,984 (48.8)
20,537 (48.9)
0.346
Male
8,372 (50.2)
21,459 (51.1)
Born prior to 37 weeks gestation
Characteristic
Childhood DFV
N (%)
No recorded childhood DFV
N (%)
p-value c
Yes
2,324 (14.2)
4,353 (10.4)
<0.0001
No
14,032 (85.8)
37,643 (89.6)
Mother’s age at birth
Characteristic
Childhood DFV
N (%)
No recorded childhood DFV
N (%)
p-value c
<20 years
4,205 (25.7)
6,122 (14.6)
<0.0001
20–29 years
9,460 (57.8)
22,774 (54.2)
30–39 years
2,591 (15.8)
12,478 (29.7)
40+ years
100 (0.6)
622 (1.5)
Father’s age at birth
Characteristic
Childhood DFV
N (%)
No recorded childhood DFV
N (%)
p-value c
<20 years
1,313 (8.0)
2,260 (5.4)
<0.0001
20–29 years
6,755 (41.3)
16,754 (39.9)
30–39 years
3,144 (19.2)
14,703 (35.0)
40+ years
590 (3.6)
2,829 (6.7)
Age missing
4,554 (27.8)
5,450 (13.0)
Maternal marital status at birth
Characteristic
Childhood DFV
N (%)
No recorded childhood DFV
N (%)
p-value c
Married/de facto/widowed
10,732 (65.6)
33,300 (79.3)
<0.0001
Never married
5,129 (31.4)
7,920 (18.9)
Divorced/separated
369 (2.3)
564 (1.3)
Unknown/not stated
126 (0.8)
212 (0.5)
Socioeconomic status
Characteristic
Childhood DFV
N (%)
No recorded childhood DFV
N (%)
p-value c
1–Most disadvantaged
8,966 (54.8)
20,569 (49.0)
<0.0001
2
3,457 (21.1)
9,549 (22.7)
3
2,236 (13.7)
6,251 (14.9)
4
1,159 (7.1)
3,857 (9.2)
5–Least disadvantaged
538 (3.3)
1,760 (4.2)
Residential remoteness
Characteristic
Childhood DFV
N (%)
No recorded childhood DFV
N (%)
p-value c
Major cities
7,079 (43.3)
20,261 (48.3)
<0.0001
Inner regional
1,485 (9.1)
4,520 (10.8)
Outer regional
2,318 (14.2)
6,725 (16.0)
Remote
2,047 (12.5)
5,190 (12.4)
Very remote
3,427 (21.0)
5,300 (12.6)
Mean age (years) of child at exposure to DFV
Characteristic
Childhood DFV
N (%)
No recorded childhood DFV
N (%)
p-value c
6.5 (SD 4.8) d
Maternal mental health contact a
Characteristic
Childhood DFV
N (%)
No recorded childhood DFV
N (%)
p-value c
Yes
7,286 (44.6)
8,788 (20.9)
<0.0001
No
9,070 (55.5)
33,208 (79.1)
Disability
Characteristic
Childhood DFV
N (%)
No recorded childhood DFV
N (%)
p-value c
Yes
2,495 (15.3)
5,071 (12.07)
<0.0001
No
13,861 (84.8)
36,925 (87.9)
Known to child protection services b
Characteristic
Childhood DFV
N (%)
No recorded childhood DFV
N (%)
p-value c
Yes
8,667 (53.0)
1,588 (3.8)
<0.0001
No
7,689 (47.0)
40,408 (96.2)
Mental health contact
Characteristic
Childhood DFV
N (%)
No recorded childhood DFV
N (%)
p-value c
Yes
3,808 (23.3)
4,602 (11.0)
<0.0001
No
12,548 (76.7)
37,394 (89.0)
Mean age (years) of mental health contact
Characteristic
Childhood DFV
N (%)
No recorded childhood DFV
N (%)
p-value c
12.5 (SD 3.6)
11.6 (SD 4.3)
<0.0001
Notes: a Mother had a mental health diagnosis in HMDC or MHIS records that occurred prior to the child’s mental health episode.
b Child has a record of notification to department for child protection and family support.
c p-value at 95 per cent level.
d SD= standard deviation.
Sociodemographic groupings may not add to 100 per cent due to rounding.
Risk of mental health service contact and mental health diagnosis in children exposed to DFV
Risk of mental health contact in children exposed to DFV
During their childhood, children exposed to DFV had an unadjusted 70 per cent increased risk of mental health contact compared to non-exposed children over the same period (Table 7). Following model adjustment, we found a statistically significant 49 per cent increased risk of mental health service contact, during childhood, for children exposed to DFV compared with non-exposed children.
Several other characteristics were found to be independently associated with mental health service contact including being Aboriginal and Torres Strait Islander, having disability, having a mother who was divorced or separated at the child’s birth, and being born to a mother over 40 years of age (Table 7).
Table 7: Adjusted and unadjusted risk of mental health service contact in childhood
Aboriginal and/or Torres Strait Islander
Characteristic
Unadjusted hazard ratios (95% CI) c
Adjusted a hazard ratios (95% CI)
Yes
1.49 (1.42, 1.56) d
1.34 (1.27, 1.42)
No
Reference group
Reference group
Sex
Characteristic
Unadjusted hazard ratios (95% CI) c
Adjusted a hazard ratios (95% CI)
Female
0.97 (0.93, 1.02)
0.99 (0.95, 1.04)
Male
Reference group
Reference group
Born prior to 37 weeks gestation
Characteristic
Unadjusted hazard ratios (95% CI) c
Adjusted a hazard ratios (95% CI)
Yes
1.36 (1.27, 1.46)
1.14 (1.07, 1.22)
No
Reference group
Reference group
Mother’s age at birth
Characteristic
Unadjusted hazard ratios (95% CI) c
Adjusted a hazard ratios (95% CI)
< 20 years
1.47 (1.37, 1.57)
1.04 (0.96, 1.14)
20–29 years
1.15 (1.08, 1.22)
0.98 (0.92, 1.05)
30–39 years
Reference group
Reference group
40+ years
1.39 (1.13, 1.72)
1.29 (1.04, 1.60)
Father’s age at birth
Characteristic
Unadjusted hazard ratios (95% CI) c
Adjusted a hazard ratios (95% CI)
< 20 years
1.54 (1.40, 1.70)
1.11 (0.99, 1.24)
20–29 years
1.25 (1.18, 1.32)
1.09 (1.03, 1.17)
30–39 years
Reference group
Reference group
40+ years
1.27 (1.14, 1.41)
1.23 (1.10, 1.37)
Missing age
1.75 (1.64, 1.87)
1.23 (1.14, 1.34)
Maternal marital status at birth
Characteristic
Unadjusted hazard ratios (95% CI) c
Adjusted a hazard ratios (95% CI)
Married/de facto/widowed
Reference group
Reference group
Never married
1.45 (1.38, 1.52)
1.13 (1.07, 1.20)
Divorced/separated
1.70 (1.45, 1.99)
1.36 (1.16, 1.60)
Unknown/not stated
2.23 (1.74, 2.86)
1.76 (1.37, 2.26)
Socioeconomic status
Characteristic
Unadjusted hazard ratios (95% CI) c
Adjusted a hazard ratios (95% CI)
1–Most disadvantaged
1.50 (1.31, 1.72)
1.31 (1.14, 1.51)
2
1.32 (1.15, 1.52)
1.25 (1.08, 1.44)
3
1.38 (1.19, 1.59)
1.31 (1.13, 1.52)
4
1.19 (1.02, 1.40)
1.21 (1.03, 1.42)
5–Least disadvantaged
Reference group
Reference group
Residential remoteness
Characteristic
Unadjusted hazard ratios (95% CI) c
Adjusted a hazard ratios (95% CI)
Major cities
1.07 (0.98, 1.15)
1.06 (0.97, 1.14)
Inner regional
Reference group
Reference group
Outer regional
1.04 (0.95, 1.15)
0.96 (0.88, 1.06)
Remote
1.17 (1.06, 1.28) d
1.00 (0.91, 1.11)
Very remote
1.10 (1.00, 1.20)
0.81 (0.74, 0.89)
Maternal mental health contact b
Characteristic
Unadjusted hazard ratios (95% CI) c
Adjusted a hazard ratios (95% CI)
Yes
1.41 (1.35, 1.48)
1.16 (1.11, 1.22)
No
Reference group
Reference group
DFV during childhood
Characteristic
Unadjusted hazard ratios (95% CI)c
Adjusted a hazard ratios (95% CI)
Yes
1.70 (1.62, 1.78)
1.49 (1.42, 1.57)
No
Reference group
Reference group
Child has disability
Characteristic
Unadjusted hazard ratios (95% CI) c
Adjusted a hazard ratios (95% CI)
Yes
1.77 (1.67, 1.87)
1.67 (1.58, 1.77)
No
Reference group
Reference group
Notes: a Multivariate analysis adjusted for all characteristic variables in table.
b Mother had a mental health diagnosis in HMDC, EDDC or MHIS records that occurred prior to the child’s mental health contact.
c CI = confidence interval.
d Bold text denotes statistically significant estimates where the 95 per cent CIs did not include the null value.
Mental health diagnosis in children exposed to DFV
Many children who were using mental health services had no formal mental health diagnosis captured in mental health services or hospital data – specifically, 12 per cent of children exposed to DFV and 6 per cent of non-exposed children. To gain an insight into the impact DFV exposure has on children’s mental health, we investigated 10 subcategories of mental health (Figure 2). Details of adjusted hazard ratios presented can be found in Appendix B.
Following model adjustment, we found that children exposed to DFV had a 19 to 99 per cent higher risk of having a diagnosis in eight of the 10 subcategories compared to their non-exposed peers (Figure 2), with only the categories “organic disorder” and “other mental illness-related contacts” showing no significant risk increase.
As shown in Figure 2, children exposed to DFV had a two-fold increased risk of substance use disorder, a 76 per cent increased risk of personality disorder and a 59 per cent increased risk of self-harm compared to non-exposed children. We also found that children exposed to DFV had a 49 per cent increased risk of anxiety disorder and a 39 per cent increased risk of schizophrenia compared with non-exposed children.
Figure 2: Risk of child with DFV exposure having a mental health subcategory diagnosis compared to non-exposed children
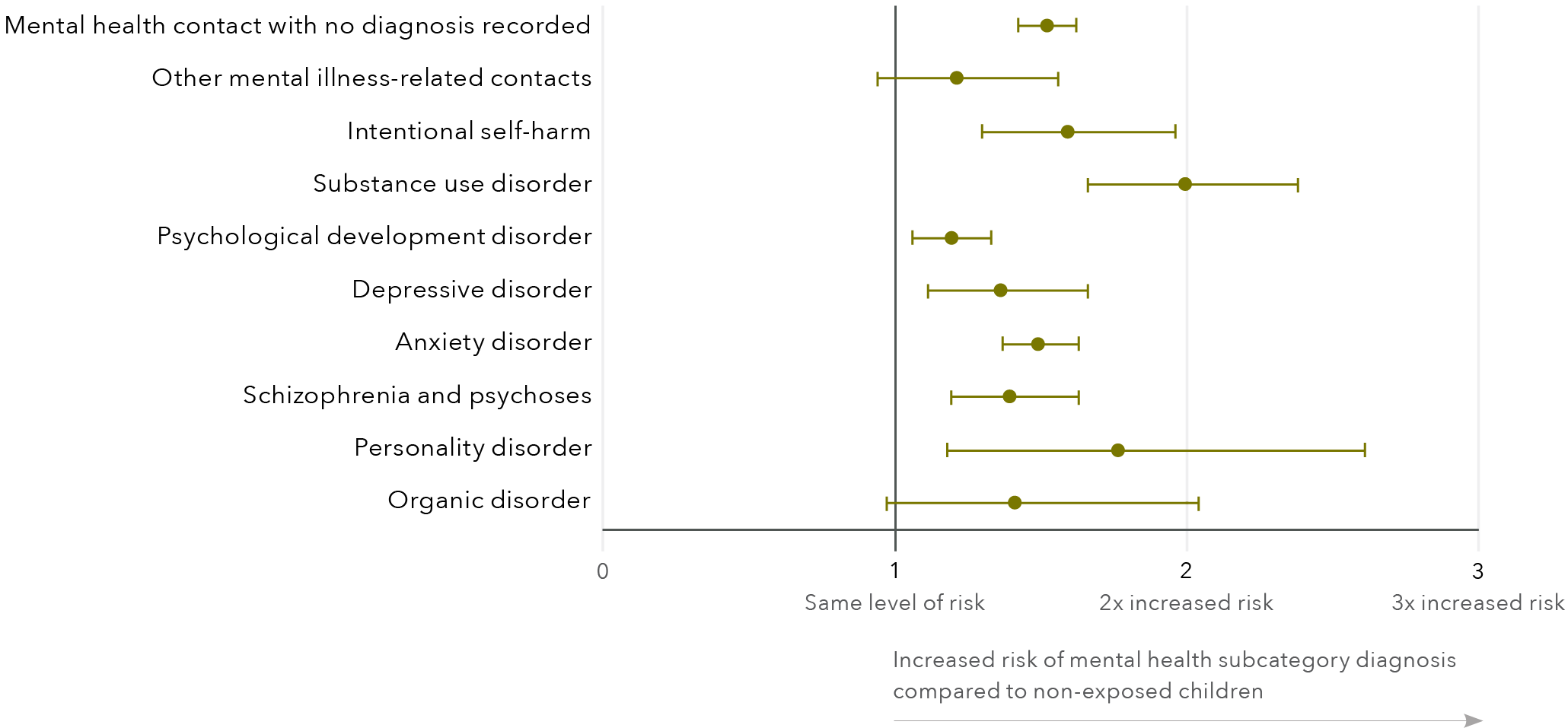
Mental health subcategory
Adjusted hazard ratios (95% CI)
Mental health contact with no diagnosis record
1.52 (1.42, 1.62)
Other mental illness-related contacts
1.21 (0.94, 1.56)
Intentional self-harm
1.59 (1.30, 1.96)
Substance use disorder
1.99 (1.66, 2.38)
Psychological development disorder
1.19 (1.06, 1.33)
Depressive disorder
1.36 (1.11, 1.66)
Anxiety disorder
1.49 (1.37, 1.63)
Schizophrenia and psychoses
1.39 (1.19, 1.63)
Personality disorder
1.76 (1.18, 2.61)
Organic disorder
1.41 (0.97, 2.04)
Note: Risk calculated using adjusted hazard ratios. Individual models were run for each subcategory. Models were adjusted for Aboriginal and Torres Strait Islander status, sex, early gestation (<37 weeks), mother’s age at birth, father’s age at birth, maternal marital status at birth, SES, residential remoteness, disability and maternal mental health contact. Error bars denote 95 per cent confidence intervals.S
Characteristics associated with mental health service contact and diagnosis
Characteristics associated with increased risk of mental health service contact
Table 8 shows the results from multivariate modelling examining the association between characteristics and mental health service contact in exposed and non-exposed children.
Aboriginal and Torres Strait Islander children in the exposed group had a 25 per cent increased risk of mental health service contact, while there was a 35 per cent increased risk of mental health service contact in non-exposed Aboriginal and Torres Strait Islander children. For children exposed to DFV, having disability was associated with a 41 per cent significantly increased risk of mental health service contact compared to children exposed to DFV with no disability. However, in non-exposed children with disability a significantly increased risk of 88 per cent was seen when compared to non-exposed children without disability.
In children exposed to DFV, having a mother under 30 years of age was associated with a 16 to 17 per cent reduced risk of mental health service contact when compared to children exposed to DFV born to a mother aged 30 to 39. This is in contrast to the non-exposed children, where being born to a teenage mother increased the risk of mental health service contact by 20 per cent when compared to non-exposed children born to a mother aged 30 to 39. Additionally, for non-exposed children, being born to a mother aged 20 to 29 had no significant impact on risk when compared to non-exposed children born to a mother aged 30 to 39. Maternal mental health contact did not increase the risk of mental health service contact for children exposed to DFV when compared to children exposed to DFV whose mother had no mental health service contact. Conversely, it was associated with a 34 per cent significantly increased risk in non-exposed children when compared tonon-exposed children whose mother had no mental health service contact.
Low SES was associated with an increased risk of mental health service contact in non-exposed children, when compared to least disadvantaged SES children who were not exposed. However, low SES was not associated with mental health service contact in children exposed to DFV when compared to least disadvantaged SES children not exposed to DFV.
Table 8: Risk of mental health service contact in childhood for children exposed to DFV and children not exposed to DFV
Aboriginal and/or Torres Strait Islander
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Yes
1.25 (1.15, 1.37) c
1.35 (1.25, 1.45)
No
Reference group
Reference group
Sex
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Female
1.02 (0.95, 1.10)
0.98 (0.92, 1.04)
Male
Reference group
Reference group
Born prior to 37 weeks gestation
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Yes
1.17 (1.06, 1.29)
1.11 (1.01, 1.22)
No
Reference group
Reference group
Mother’s age at birth
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
<20 years
0.83 (0.72, 0.95)
1.20 (1.07, 1.34)
20–29 years
0.84 (0.75, 0.94)
1.04 (0.96, 1.13)
30–39 years
Reference group
Reference group
40+ years
1.26 (0.82, 1.92)
1.30 (1.01, 1.67)
Father’s age at birth
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
< 20 years
1.09 (0.92, 1.29)
1.09 (0.94, 1.27)
20–29 years
1.13 (1.01, 1.26)
1.05 (0.97, 1.14)
30–39 years
Reference group
Reference group
40+ years
1.31 (1.07, 1.61)
1.19 (1.04, 1.36)
Missing age
1.23 (1.09, 1.39)
1.22 (1.10, 1.36)
Maternal marital status at birth
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Married/de facto/widowed
Reference group
Reference group
Never married
1.05 (0.97, 1.14)
1.19 (1.10, 1.29)
Divorced/separated
1.11 (0.88, 1.42)
1.54 (1.25, 1.91)
Unknown/not stated
1.81 (1.27, 2.59)
1.68 (1.17, 2.39)
Socioeconomic status
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
1–Most disadvantaged
1.06 (0.86, 1.31)
1.51 (1.25, 1.83)
2
1.02 (0.83, 1.27)
1.43 (1.18, 1.73)
3
1.19 (0.96, 1.49)
1.42 (1.16, 1.73)
4
1.05 (0.82, 1.33)
1.34 (1.09, 1.66)
5–Least disadvantaged
Reference group
Reference group
Residential remoteness
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Major cities
1.11 (0.97, 1.27)
1.02 (0.92, 1.13)
Inner regional
Reference group
Reference group
Outer regional
1.00 (0.85, 1.16)
0.95 (0.84, 1.06)
Remote
1.03 (0.87, 1.20)
0.98 (0.87, 1.11)
Very remote
0.81 (0.69, 0.94)
0.81 (0.71, 0.92)
Maternal mental health contact
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Yes
0.94 (0.88, 1.02)
1.34 (1.26, 1.43)
No
Reference group
Reference group
Child has disability
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Yes
1.41 (1.28, 1.54)
1.88 (1.74, 2.02)
No
Reference group
Reference group
Notes: a Adjusted for characteristics listed in table.
b Mother had a mental health diagnosis in HMDC or MHIS records that occurred prior to the child’s mental health contact.
c Bold text denotes statistically significant estimates where the 95 per cent CIs did not include the null value.
Characteristics associated with increased risk of mental health subtypes
Characteristics that were associated with an increased risk of mental health subtypes for children exposed to DFV are displayed in Table 9. The table only displays characteristics that were significantly associated with increased risk. The full set of results of all sociodemographic characteristics, stratified by DFV exposure, can be found in Appendix C.
For children exposed to DFV, being Aboriginal and Torres Strait Islander was associated with a significantly increased risk of substance use disorder of 192 per cent. For non-exposed children, being Aboriginal and Torres Strait Islander was correlated with a 360 per cent increased risk of substance use disorder (see Appendix C for all non-exposed results).
Being female was associated with a significantly increased risk of diagnosis in six of the mental health diagnostic subcategories for children exposed to DFV, ranging from a 36 per cent increased risk of anxiety disorder to a significantly increased risk (183%) of depressive disorder. Similarly, non-exposed female children also had a significantly increased risk in the same six subcategories, ranging from 48 per cent for anxiety disorder and personality disorder to 220 per cent for intentional self-harm.
Having disability was associated with a significant increase in the risk of a diagnosis in nine of the 10 mental disorder subcategories for children exposed to DFV. This association ranged from a 31 per cent increase in anxiety disorder to a 180 per cent increase in substance use disorder. Similarly, having disability was associated with an increased risk in seven of the 10 subcategories in non-exposed children, ranging from 61 per cent in anxiety disorder and personality disorder to 228 per cent in psychological development disorder.
Table 9: Association of sociodemographic characteristics on the risk of childhood mental health diagnosis by subcategory in children exposed to DFV
Sociodemographic characteristics
Anxiety disorder
Psychological development
Substance use disorder
Schizophrenia and psychoses
Intentional self-harm
Depressive disorder
Organic disorder
Personality disorder
Other mental illness-related contacts
Mental health contact with no diagnosis recorded
Aboriginal and Torres Strait Islander
192%
Grey shading
Female
36%
Grey shading
95%
Grey shading
181%
Grey shading
183%
Amber shading
100%
Amber shading
100%
Grey shading
Born prior to 37 weeks gestation
35%
Amber shading
19%
Amber shading
Father’s age at birth 20–29 years
31%
Amber shading
Father’s age at birth missing a
45%
Amber shading
89%
Amber shading
Maternal marital status at birth: divorced/separated
36%
Grey shading
ARIA: major city
48%
Amber shading
Child has disability
31%
Grey shading
167%
Grey shading
180%
Amber shading
53%
Amber shading
55%
Amber shading
72%
Amber shading
113%
Amber shading
149%
Amber shading
149%
Amber shading
Notes: a Father’s age at birth missing in Midwives Notification System.
Models were adjusted for Aboriginal and Torres Strait Islander status, sex, early gestation (<37 weeks), mother’s age at birth, father’s
age at birth, maternal marital status at birth, SES, residential remoteness, disability and maternal mental health contact.
Grey shading indicates that the associated risk is lower than that observed in children not exposed to DFV. Amber shading indicates the associated risk is greater than observed in children not exposed to DFV.
Mental health service use and trajectories of children exposed to DFV
Probability of mental health service contact in childhood by DFV exposure
Figure 3 displays the cumulative probability of mental health service contact over time for children exposed to DFV and children not exposed. The cumulative probability of having a mental health service contact was higher for children exposed to DFV, who had a 78.6 per cent chance of having a mental health contact by age 18. For children not exposed to DFV the cumulative probability of having a mental health service contact was 15.9 per cent by age 18.
Figure 3: Cumulative probability of mental health service contact over time by DFV exposure
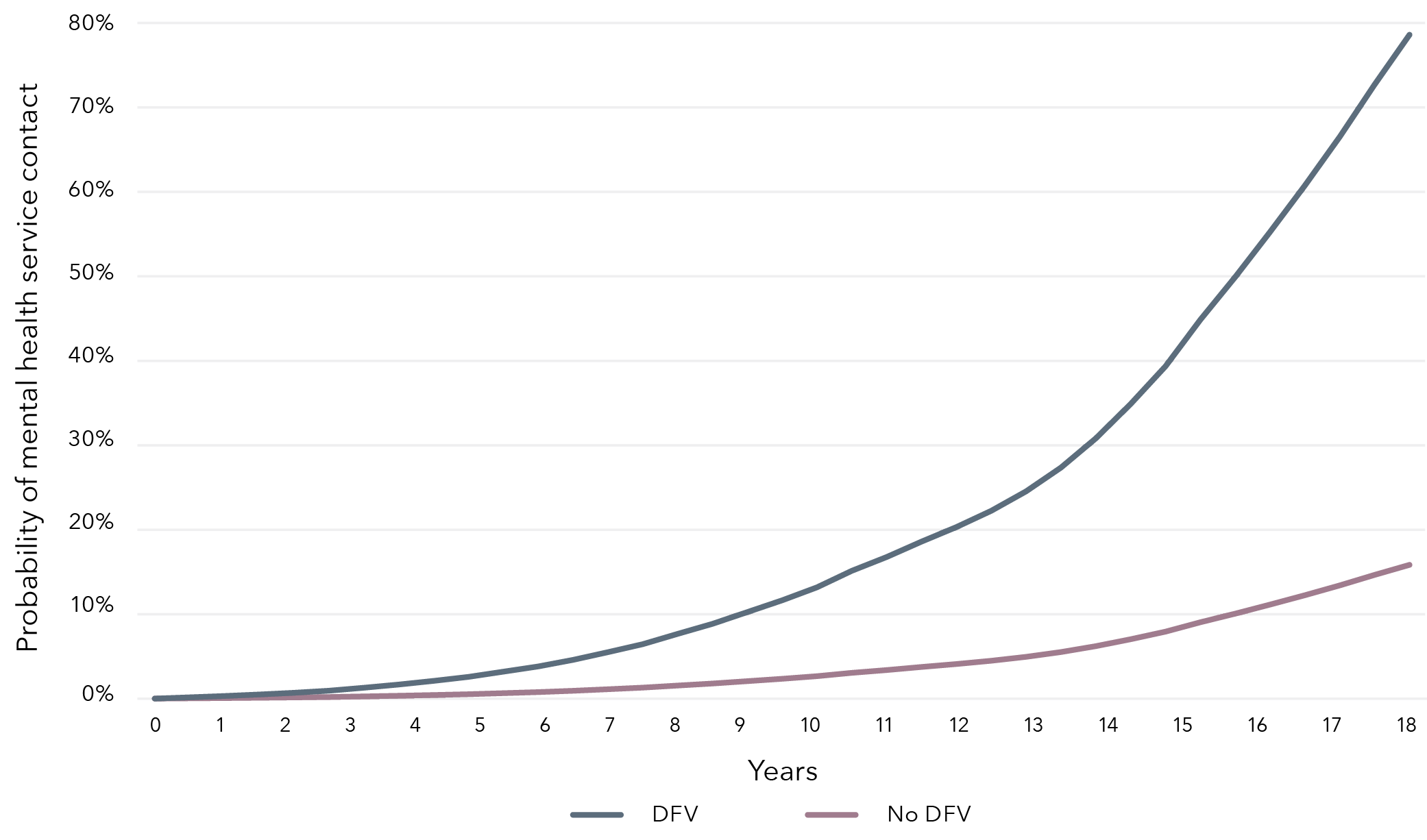
Note: Differences in cumulative probability between children exposed and not exposed to DFV: Gray’s p-value<0.0001.
Probability of mental health service contact in childhood by sex and DFV exposure
Prior to 15 years of age, male children exposed to DFV had the highest probability of a mental health service contact with 17.5 per cent cumulative probability (Figure 4). However, at the end of follow-up, the cumulative probability of having a mental health service contact was highest in female children exposed to DFV: they had a 30.5 per cent chance of having a mental health service contact by 18 years of age, which is slightly higher than the 28 per cent cumulative probability seen in males at the same time point.
Figure 4: Cumulative probability of mental health service contact over time by exposure status and sex
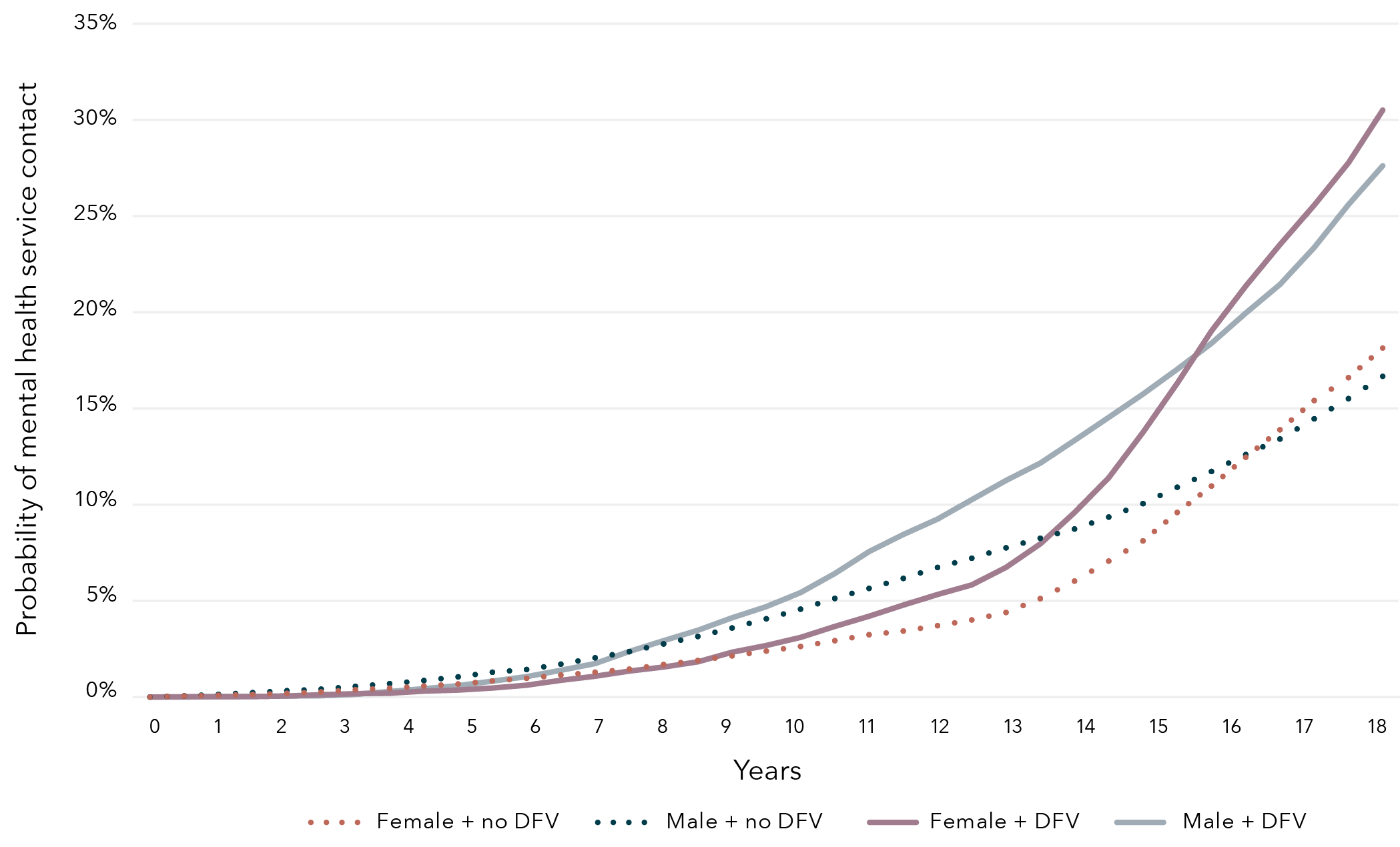
Notes: Differences in cumulative probability between non-exposed female and non-exposed male: Gray’s p=0.0748.
Differences in cumulative probability between exposed female and exposed male: Gray’s p=0.9367.
Probability of mental health service contact in childhood by SES and DFV exposure
Figure 5 displays the cumulative probability of having a mental health service contact by 18 years of age, stratified by SES and DFV exposure. Due to low counts within the initial quintiles of SES, the categories were collapsed to “lowest 20 per cent disadvantage” (i.e. the lowest 20th percentile of most disadvantaged) and “upper 80 per cent of disadvantage” (i.e. the upper 80th percentile of least disadvantaged). There was minimal difference between the trajectories for lower and upper disadvantage groups, with the most variation observed within the non-exposure group. The cumulative probability of having a mental health service contact by 18 years was 28.7 per cent for those exposed to DFV, irrespective of their SES status.
Figure 5: Cumulative probability of mental health service contact over time by exposure status and socioeconomic status
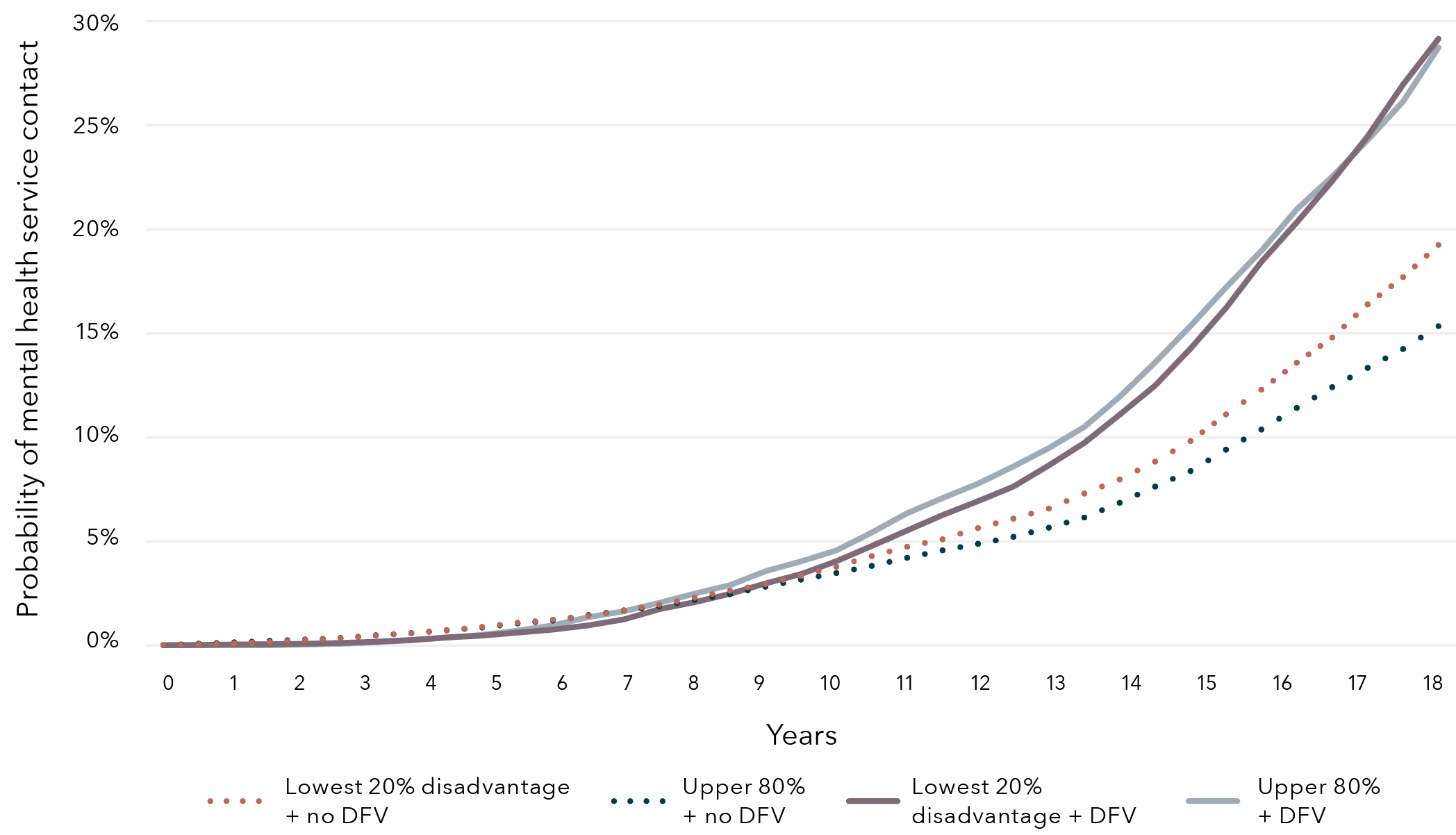
Notes: Differences in cumulative probability between least and most disadvantaged non-exposed children: Gray’s p<0.0001.
Differences in cumulative probability between least and most disadvantaged children exposed to DFV: Gray’s p=0.8011.
Probability of mental health service contact in childhood by disability status and DFV exposure
The comparison of children with and without disability and their cumulative probability of having a mental health service contact by exposure status is shown in Figure 6. Until age 10, children with disability and no DFV exposure had the highest probability of mental health service contact of all four groups. However, after 10 years of age, children with disability who were exposed to DFV had the highest cumulative probability of a mental health service contact: 36.3 per cent by the time they reach 18.
For children without disability, the cumulative probability of mental health service contact was similar until around age 9, after which point the trajectory increased more rapidly in children exposed to DFV. By age 18, non-exposed children without disability had a 16.3 per cent likelihood of mental health service contact whereas children exposed to DFV without disability had a 27.7 per cent cumulative probability of mental health service contact.
Figure 6: Cumulative probability of mental health service contact over time by exposure status and disability
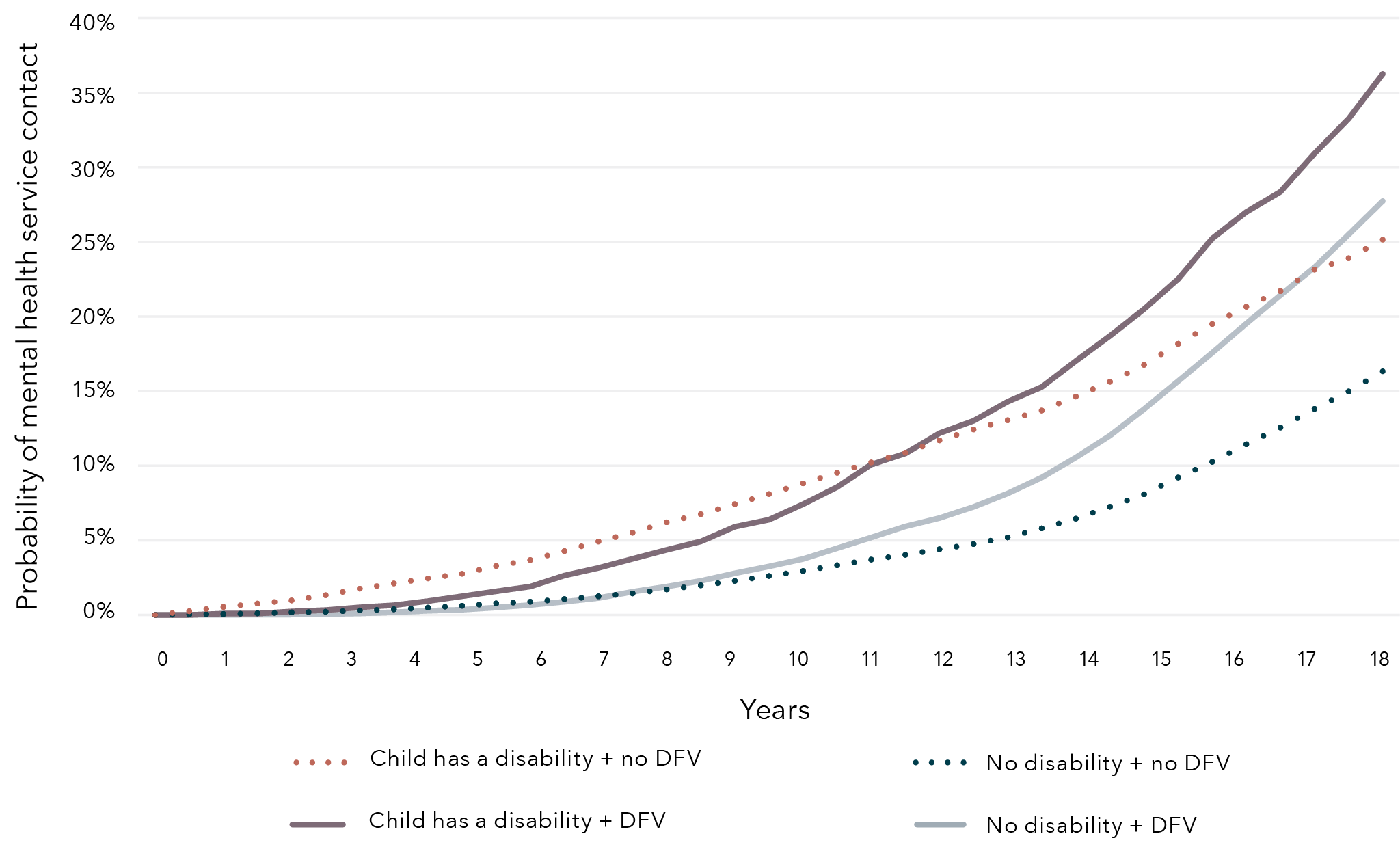
Notes: Differences in cumulative probability between non-exposed children with disability and without: Gray’s p<0.0001.
Differences in cumulative probability between children exposed to DFV with disability and without: Gray’s p<0.0001.
Probability of mental health service contact in childhood by Aboriginal and Torres Strait Islander status and DFV exposure
Prior to 12 years of age, non-Aboriginal and Torres Strait Islander children exposed to DFV had the highest cumulative probability of mental health service contact: 8.8 per cent of the four groups (Figure 7). However, over time, the cumulative probability of having a mental health service contact is highest for Aboriginal and Torres Strait Islander children exposed to DFV, who had a 31.6 per cent probability of having a mental health service contact by 18. By the end of follow-up, non-Aboriginal and Torres Strait Islander children with no DFV exposure had the lowest cumulative probability of having a mental health service contact (13.2%).
Figure 7: Cumulative probability of mental health service contact over time by exposure status and Aboriginal and Torres Strait Islander status
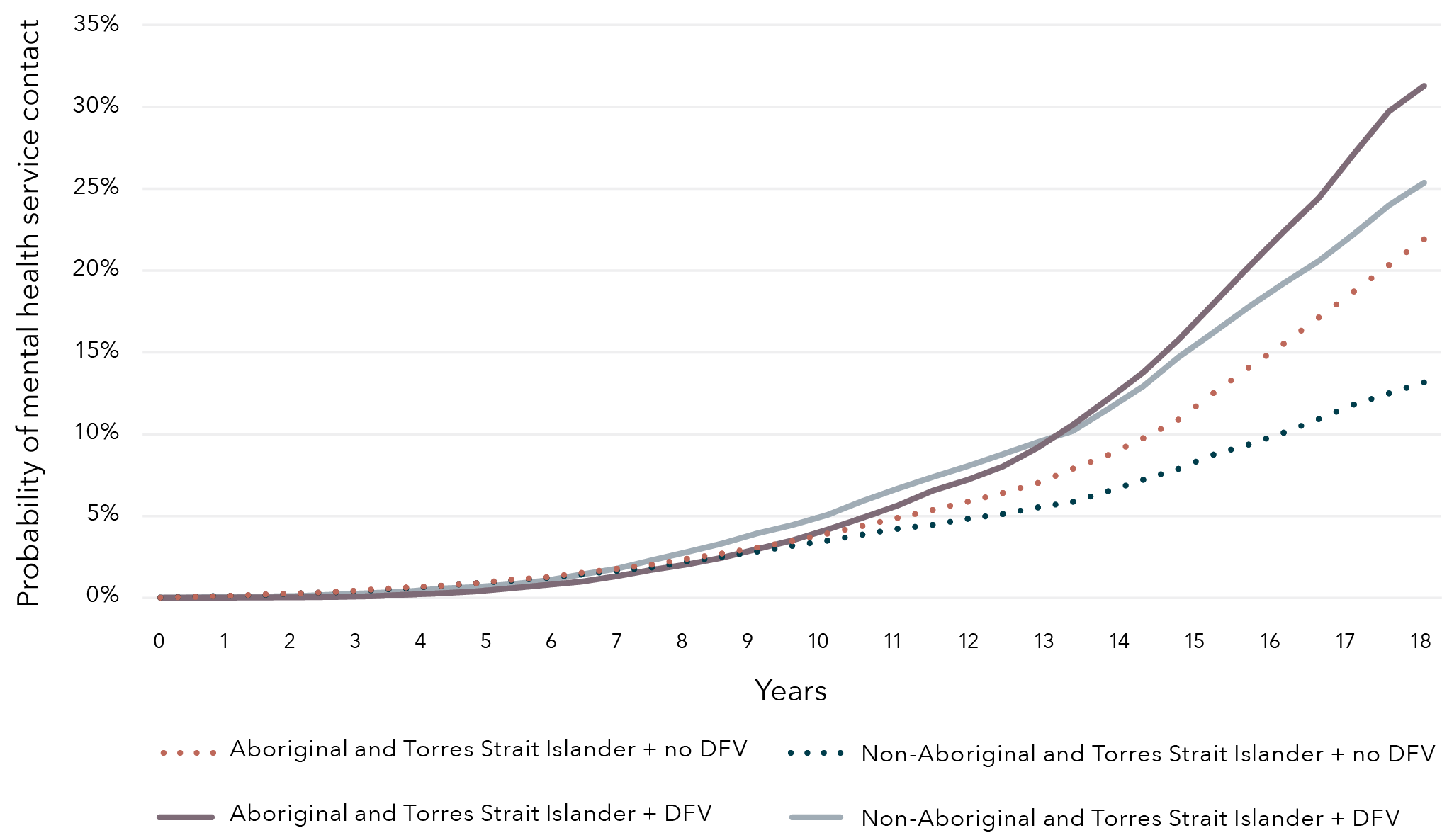
Notes: Differences in cumulative probability between Aboriginal and Torres Strait Islander children with and without exposure: Gray’s p<0.0001.
Differences in cumulative probability between non-Aboriginal and Torres Strait Islander children with and without exposure: Gray’s p<0.0001.
Aboriginal and Torres Strait Islander children
Characteristics associated with increased risk of mental health service contact in Aboriginal and Torres Strait Islander children
Table 10 displays the characteristics associated with mental health service contact for Aboriginal and Torres Strait Islander children exposed to DFV and Aboriginal and Torres Strait Islander children not exposed to DFV. Accounting for sociodemographic characteristics, Aboriginal and Torres Strait Islander children exposed to DFV who were born pre-term (prior to 37 weeks gestation) were 18 per cent more likely to have a mental health service contact than those born at term. Similar associated increased risk was seen in Aboriginal and Torres Strait Islander children born pre-term but not exposed to DFV.
For Aboriginal and Torres Strait Islander children exposed to DFV, being born to a mother aged under 30 was associated with a decreased risk of mental health service contact of 18 to 25 per cent, compared to those with an older mother. Conversely, maternal age was not associated with mental health service contact for non-exposed Aboriginal and Torres Strait Islander children. Being born to a father aged over 40 was associated with an increased risk of mental health service contact by 68 per cent in Aboriginal and Torres Strait Islander children exposed to DFV, compared with having a younger father. Father’s age was not associated with mental health service contact for Aboriginal and Torres Strait Islander children not exposed to DFV.
Having a mother’s marital status at birth missing or unknown in the Midwives Notification System was associated with an increased risk of mental health service contact of 75 per cent in Aboriginal and Torres Strait Islander children exposed to DFV, compared to those whose mother was married, widowed or in a de facto relationship. A similar risk increase was observed in the non-exposed children. Unlike children exposed to DFV, where no association was found, being born to a mother who was divorced was observed to increase the risk of mental health service contact by 35 per cent in Aboriginal and Torres Strait Islander children not exposed to DFV.
Being born in a major city was associated with an increased risk of mental health service contact for Aboriginal and Torres Strait Islander children exposed to DFV by 37 per cent compared with children exposed to DFV residing in inner regional areas. A 19 per cent increased risk in mental health service contact was observed in the non-exposed Aboriginal and Torres Strait Islander children residing in major cities compared to non-exposed inner regional children. Conversely, for Aboriginal and Torres Strait Islander children not exposed to DFV, residing in a very remote regional area was associated with a 16 per cent decreased risk of mental health service contact compared to those in inner regional areas. However, no significant association was seen in children exposed to DFV residing in a remote area for mental health service contact.
Being born to a mother who had a prior mental health contact was not associated with mental health service contact in children exposed to DFV. However, it was associated with a 10 per cent increase in risk of contact in non-exposed children.
For Aboriginal and Torres Strait Islander children exposed to DFV, having disability was associated with a 28 per cent greater risk of mental health service contact than Aboriginal and Torres Strait Islander children exposed to DFV who do not have disability. However, for non-exposed Aboriginal and Torres Strait Islander children, having disability was associated with a higher risk of 75 per cent, when compared to non-exposed Aboriginal and Torres Strait Islander children without disability.
Table 10: Risk of mental health service contact in childhood for Aboriginal and Torres Strait Islander children with exposure to DFV and without exposure to DFV
Sex
Characteristic
Exposed to DFV adjusted hazard ratios b (95% CI)
No DFV exposure adjusted hazard ratios (95% CI)
Female
0.97 (0.89, 1.06)
0.93 (0.86, 1.00)
Male
Reference group
Reference group
Born prior to 37 weeks gestation
Characteristic
Exposed to DFV adjusted hazard ratios b (95% CI)
No DFV exposure adjusted hazard ratios (95% CI)
Yes
1.18 (1.05, 1.33) c
1.14 (1.02, 1.28)
No
Reference group
Reference group
Mother’s age at birth
Characteristic
Exposed to DFV adjusted hazard ratios b (95% CI)
No DFV exposure adjusted hazard ratios (95% CI)
<20 years
0.75 (0.63, 0.88)
1.10 (0.96, 1.27)
20–29 years
0.82 (0.71, 0.94)
0.98 (0.88, 1.10)
30–39 years
Reference group
Reference group
40+ years
0.85 (0.42, 1.73)
1.32 (0.90, 1.92)
Father’s age at birth
Characteristic
Exposed to DFV adjusted hazard ratios b (95% CI)
No DFV exposure adjusted hazard ratios (95% CI)
<20 years
1.08 (0.88, 1.34)
1.01 (0.85, 1.20)
20–29 years
1.07 (0.92, 1.24)
0.96 (0.86, 1.08)
30–39 years
Reference group
Reference group
40+ years
1.68 (1.30, 2.18)
1.22 (0.99, 1.49)
Missing age
1.15 (0.99, 1.34)
1.17 (1.03, 1.32)
Maternal marital status at birth
Characteristic
Exposed to DFV adjusted hazard ratios b (95% CI)
No DFV exposure adjusted hazard ratios (95% CI)
Married/de facto/widowed
Reference group
Reference group
Never married
1.03 (0.93, 1.13)
1.09 (1.00, 1.20)
Divorced/separated
1.17 (0.86, 1.58)
1.35 (1.05, 1.75)
Unknown/not stated
1.75 (1.18, 2.61)
1.74 (1.19, 2.56)
Socioeconomic status
Characteristic
Exposed to DFV adjusted hazard ratios b (95% CI)
No DFV exposure adjusted hazard ratios (95% CI)
1–Most disadvantaged
0.90 (0.67, 1.21)
1.29 (0.96, 1.74)
2
0.91 (0.67, 1.24)
1.22 (0.90, 1.66)
3
1.02 (0.74, 1.39)
1.32 (0.97, 1.81)
4
1.16 (0.82, 1.64)
1.40 (1.01, 1.95)
5–Least disadvantaged
Reference group
Reference group
Residential remoteness
Characteristic
Exposed to DFV adjusted hazard ratios b (95% CI)
No DFV exposure adjusted hazard ratios (95% CI)
Major cities
1.37 (1.11, 1.68)
1.19 (1.02, 1.39)
Inner regional
Reference group
Reference group
Outer regional
1.14 (0.91, 1.42)
1.00 (0.84, 1.18)
Remote
1.16 (0.93, 1.45)
1.01 (0.86, 1.20)
Very remote
0.94 (0.77, 1.16)
0.84 (0.72, 0.99)
Maternal mental health contact a
Characteristic
Exposed to DFV adjusted hazard ratios b (95% CI)
No DFV exposure adjusted hazard ratios (95% CI)
Yes
0.87 (0.79, 0.95)
1.10 (1.02, 1.20)
No
Reference group
Reference group
Child has disability
Characteristic
Exposed to DFV adjusted hazard ratios b (95% CI)
No DFV exposure adjusted hazard ratios (95% CI)
Yes
1.28 (1.14 1.43)
1.75 (1.59, 1.93)
No
Reference group
Reference group
Notes: a Mother had a mental health diagnosis in HMDC or MHIS records that occurred prior to the child’s mental health episode.
b Multivariate analysis adjusted for all characteristic variables in table.
c Bold text denotes statistically significant estimates where the 95 per cent CIs did not include the null value.
Subcategories of mental health diagnosis
Aboriginal and Torres Strait Islander children
Following model adjustment, we observed that Aboriginal and Torres Strait Islander children exposed to DFV had a significantly higher risk of having a diagnosis in six of the 10 subcategories compared to their non-exposed peers (Figure 8), with significant risk increases ranging from 33 per cent for schizophrenia to 85 per cent for substance use. A 67 per cent increased risk of self-harm diagnosis was seen in Aboriginal and Torres Strait Islander children exposed to DFV compared with non-exposed Aboriginal and Torres Strait Islander children. Details of adjusted hazard ratios presented in Figure 8 can be found in Appendix D.
Figure 8: Risk of Aboriginal and Torres Strait Islander child with DFV exposure having a mental health subcategory compared to non-exposed Aboriginal and Torres Strait Islander children
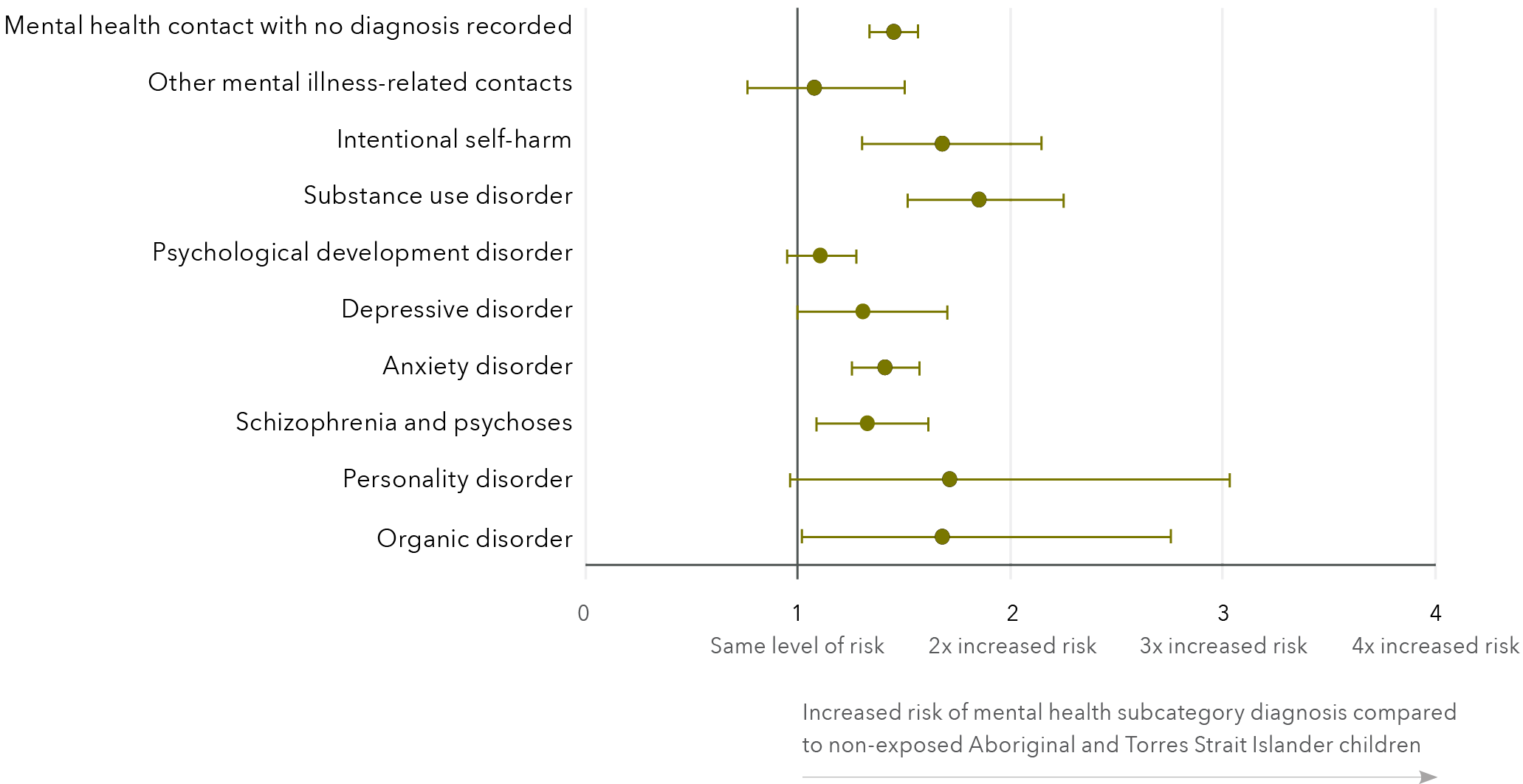
Mental health subcategory
Adjusted hazard ratios (95% CI)
Mental health contact with no diagnosis record
1.45 (1.34, 1.57)
Other mental illness-related contacts
1.07 (0.77, 1.51)
Intentional self-harm
1.67 (1.31, 2.15)
Substance use disorder
1.85 (1.52, 2.25)
Psychological development disorder
1.10 (0.95, 1.27)
Depressive disorder
1.30 (1.00, 1.70)
Anxiety disorder
1.40 (1.25, 1.58)
Schizophrenia and psychoses
1.33 (1.09, 1.61)
Personality disorder
1.71 (0.96, 3.03)
Organic disorder
1.68 (1.02, 2.76)
Notes: Individual models were run for each subcategory. Models were adjusted for sex, early gestation (<37 weeks), mother’s age at birth, father’s age at birth, maternal marital status at birth, SES, residential remoteness, disability and maternal mental health contact. Risk estimates are presented as hazard ratios; error bars denote 95 per cent confidence intervals.
Non-Aboriginal and Torres Strait Islander children
Non-Aboriginal and Torres Strait Islander children exposed to DFV were observed to have a significantly higher risk of having a diagnosis in five of the 10 subcategories compared to their non-exposed peers, ranging from 22 per cent for psychological development to 148 per cent for substance use disorder (Figure 9). Details of adjusted hazard ratios presented in Figure 9 can be found in Appendix D.
Figure 9: Risk of non-Aboriginal and/or Torres Strait Islander child with DFV exposure having a mental health subcategory compared to non-exposed, non-Aboriginal and Torres Strait Islander children
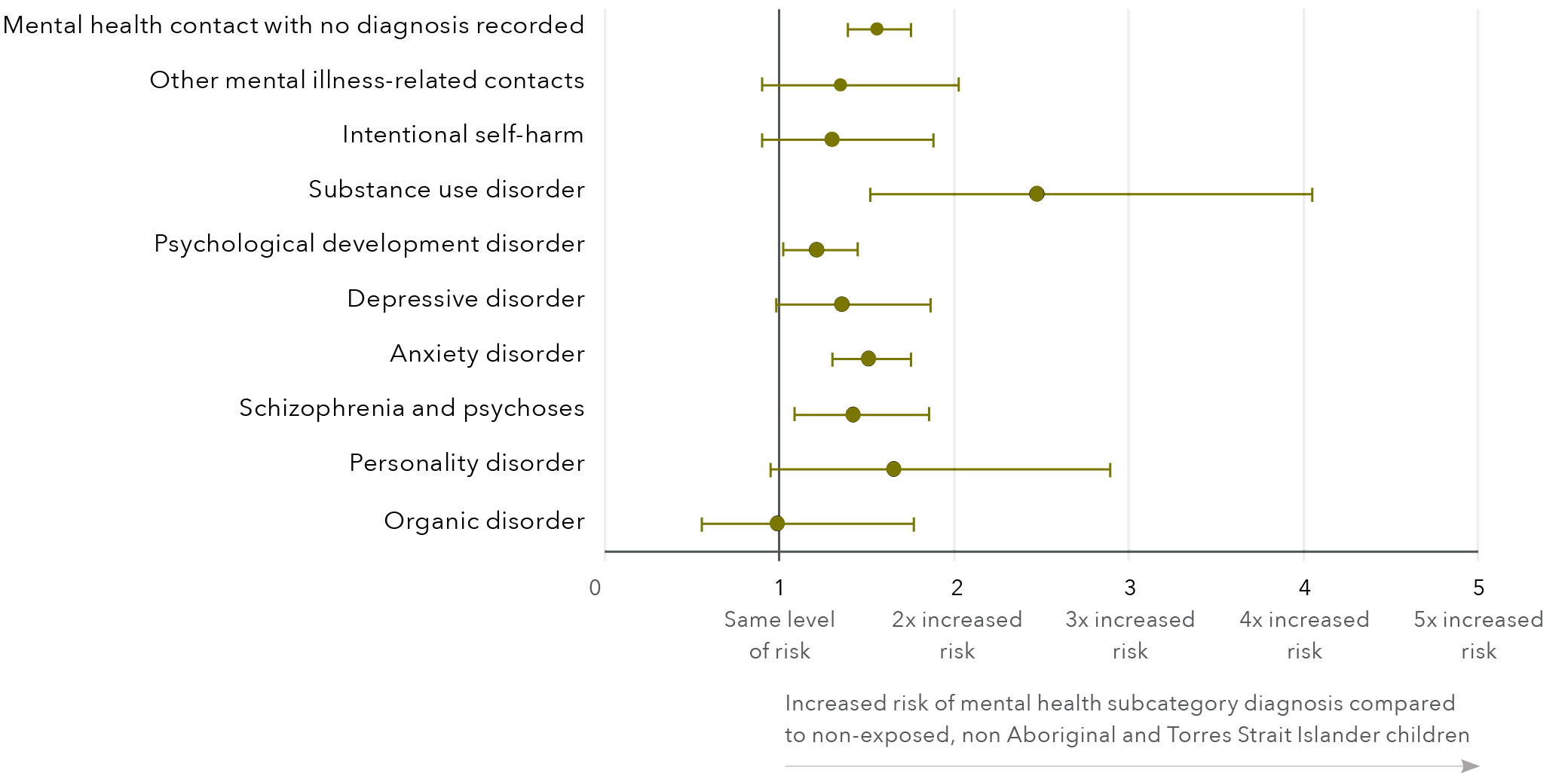
Mental health subcategory
Adjusted hazard ratios (95% CI)
Mental health contact with no diagnosis record
1.56 (1.39, 1.75)
Other mental illness-related contacts
1.35 (0.90, 2.03)
Intentional self-harm
1.30 (0.90, 1.88)
Substance use disorder
2.48 (1.52, 4.05)
Psychological development disorder
1.22 (1.02, 1.45)
Depressive disorder
1.36 (0.99, 1.87)
Anxiety disorder
1.51 (1.31, 1.75)
Schizophrenia and psychoses
1.42 (1.09, 1.86)
Personality disorder
1.66 (0.95, 2.89)
Organic disorder
0.99 (0.55, 1.77)
Notes: Individual models were run for each subcategory. Models were adjusted for sex, early gestation (<37 weeks), mother’s age at birth, father’s age at birth, maternal marital status at birth, SES, residential remoteness, disability and maternal mental health contact. Risk estimates are presented as hazard ratios; error bars denote 95 per cent confidence intervals.
Disability
Characteristics associated with increased risk of mental health service contact in children with disability
Table 11 displays the characteristics associated with mental health service contact for both children with disability who are exposed to DFV and children with disability who are not exposed to DFV. Accounting for sociodemographic characteristics, children with disability exposed to DFV who were born pre-term (prior to 37 weeks gestation) were 23 per cent more likely to have a mental health service contact than DFV-exposed children born at term. Being born early was not associated with mental health service contact in children with disability not exposed to DFV.
For a child with disability and who was exposed to DFV, being born to a father aged over 40 years was associated with a 78 per cent increased risk of mental health service contact, compared with their DFV-exposed peers born to a father aged 30–39 years. However, father’s age was not associated with the risk of mental health service contact in children with disability but not exposed to DFV.
Maternal marital status at birth being unknown or missing in the Midwives Notification System was associated with a 116 per cent increase in the risk of mental health service contact in children with disability exposed to DFV compared to those DFV-exposed children with disability whose mother was married, widowed or in a de facto relationship. However, for children with disability who were not exposed to DFV the associated risk was 179 per cent. For children with disability who were not exposed to DFV, being born to a mother who was never married was associated with a 27 per cent increased risk of mental health service contact compared to non-exposed children with disability born to a mother who was married, widowed or in a de facto relationship. For children with disability who were exposed to DFV, being born to a mother who was never married had no observed relationship with risk of mental health service contact.
SES was not associated with the risk of mental health service contact in children with disability exposed to DFV. However, being from the most disadvantaged SES and from the second-most advantaged SES was associated with an increased risk of mental health service contact in children with disability not exposed to DFV (67% and 70% respectively).
Table 11: Risk of mental health service contact in childhood for children with disability and exposure to DFV and children with disability without exposure to DFV
Aboriginal and/or Torres Strait Islander
Characteristic
Exposed to DFV adjusted hazard ratios b (95% CI)
No DFV exposure adjusted hazard ratios (95% CI)
Yes
1.13 (0.92, 1.38)
1.27 (1.08, 1.50) c
No
Reference group
Reference group
Sex
Characteristic
Exposed to DFV adjusted hazard ratios b (95% CI)
No DFV exposure adjusted hazard ratios (95% CI)
Female
0.86 (0.73, 1.02)
0.91 (0.80, 1.05)
Male
Reference group
Reference group
Born prior to 37 weeks gestation
Characteristic
Exposed to DFV adjusted hazard ratios b (95% CI)
No DFV exposure adjusted hazard ratios (95% CI)
Yes
1.23 (1.02, 1.49)
0.98 (0.82, 1.18)
No
Reference group
Reference group
Mother’s age at birth
Characteristic
Exposed to DFV adjusted hazard ratios b (95% CI)
No DFV exposure adjusted hazard ratios (95% CI)
<20 years
0.78 (0.58, 1.05)
1.22 (0.94, 1.58)
20–29 years
0.87 (0.69, 1.10)
1.08 (0.90, 1.29)
30–39 years
Reference group
Reference group
40+ years
0.96 (0.42, 2.21)
1.57 (0.98, 2.51)
Father’s age at birth
Characteristic
Exposed to DFV adjusted hazard ratios b (95% CI)
No DFV exposure adjusted hazard ratios (95% CI)
<20 years
1.21 (0.79, 1.85)
0.86 (0.59, 1.26)
20–29 years
1.37 (1.05, 1.78)
0.98 (0.82, 1.18)
30–39 years
Reference group
Reference group
40+ years
1.78 (1.18, 2.69)
1.08 (0.81, 1.43)
Missing age
1.44 (1.08, 1.91)
1.13 (0.89, 1.42)
Maternal marital status at birth
Characteristic
Exposed to DFV adjusted hazard ratios b (95% CI)
No DFV exposure adjusted hazard ratios (95% CI)
Married/de facto/widowed
Reference group
Reference group
Never married
1.06 (0.88, 1.28)
1.27 (1.06, 1.52)
Divorced/separated
0.93 (0.53, 1.62)
1.44 (0.89, 2.32)
Unknown/not stated
2.16 (1.01, 4.59)
2.79 (1.48, 5.26)
Socioeconomic status
Characteristic
Exposed to DFV adjusted hazard ratios b (95% CI)
No DFV exposure adjusted hazard ratios (95% CI)
1–Most disadvantaged
1.48 (0.91, 2.42)
1.67 (1.04, 2.70)
2
1.43 (0.86, 2.37)
1.60 (0.98, 2.60)
3
1.38 (0.82, 2.31)
1.50 (0.91, 2.46)
4
1.69 (0.97, 2.95)
1.70 (1.02, 2.83)
5–Least disadvantaged
Reference group
Reference group
Residential remoteness
Characteristic
Exposed to DFV adjusted hazard ratios b (95% CI)
No DFV exposure adjusted hazard ratios (95% CI)
Major cities
1.39 (0.98, 1.96)
0.90 (0.72, 1.13)
Inner regional
Reference group
Reference group
Outer regional
1.18 (0.79, 1.76)
0.95 (0.73, 1.24)
Remote
1.11 (0.73, 1.70)
0.85 (0.63, 1.13)
Very remote
0.83 (0.56, 1.22)
0.75 (0.56, 1.00)
Maternal mental health contact a
Characteristic
Exposed to DFV adjusted hazard ratios b (95% CI)
No DFV exposure adjusted hazard ratios (95% CI)
Yes
0.96 (0.82, 1.14)
1.16 (1.00, 1.35)
No
Reference group
Reference group
Notes: a Mother had a mental health diagnosis in HMDC or MHIS records that occurred prior to the child’s mental health episode.
b Multivariate analysis adjusted for all characteristic variables in table.
c Bold text denotes statistically significant estimates where the 95 per cent CIs did not include the null value.
Subcategories of mental health diagnosis
In children with disability, exposure to DFV was associated with an increased risk of diagnosis in all mental health subcategories when compared to non-exposed children with disability (Figures 10 & 11). The level of risk increase ranged from 53 per cent for psychological development diagnosis to 74 per cent for personality disorder. Similarly, in children without disability, exposure to DFV was associated with an increased risk of diagnosis for all subcategories compared to non-exposed peers, ranging from 88 per cent for no diagnosis to 105 per cent increased risk in organic disorders and personality disorders. Further details of adjusted hazard ratios presented can be found in Appendix E.
Figure 10: Risk of children with disability exposed to DFV having a mental health subcategory compared to non-exposed children with disability
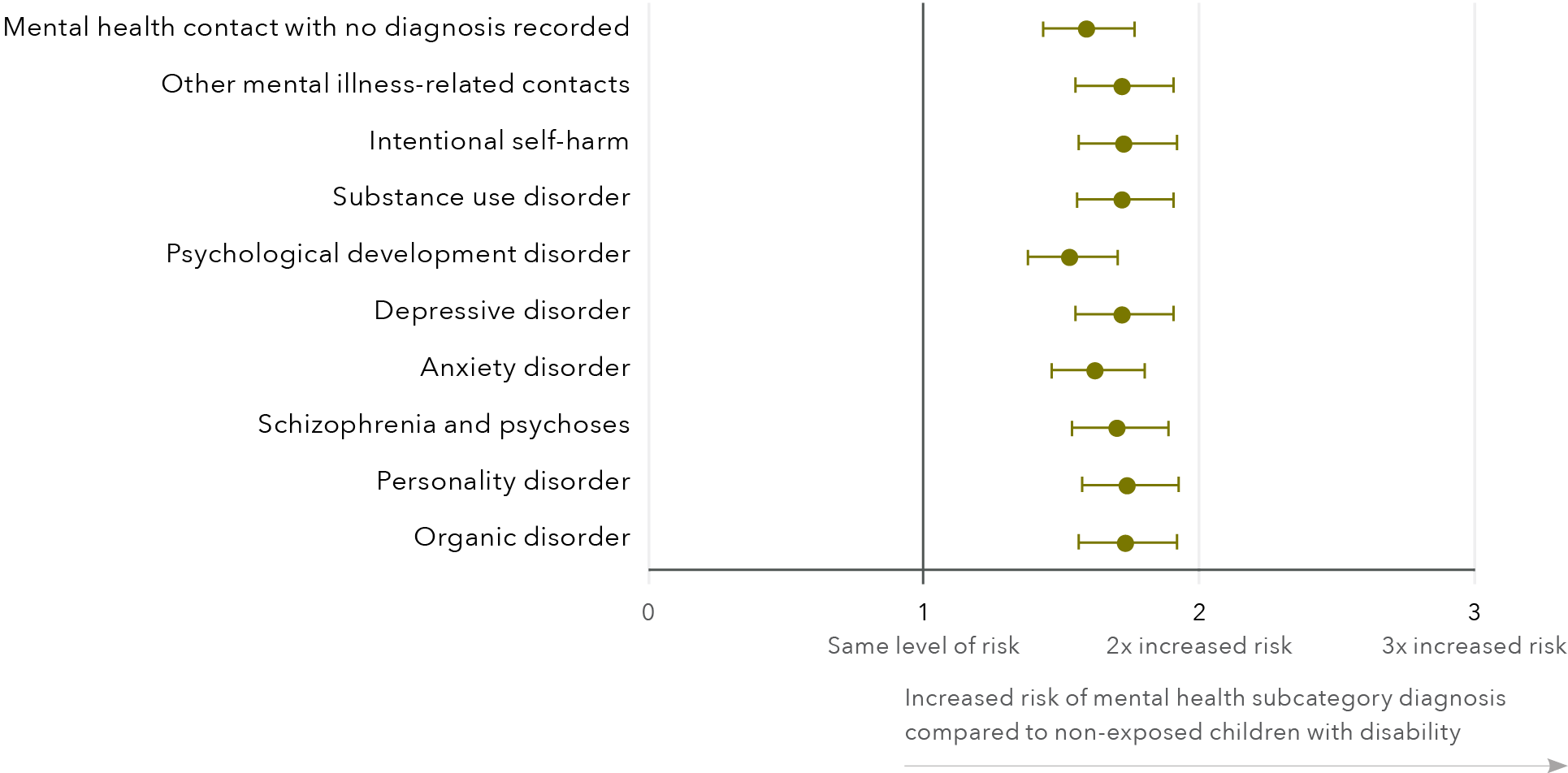
Mental health subcategory
Adjusted hazard ratios (95% CI)
Mental health contact with no diagnosis record
1.59 (1.44, 1.77)
Other mental illness-related contacts
1.72 (1.55, 1.91)
Intentional self-harm
1.73 (1.56, 1.92)
Substance use disorder
1.72 (1.56, 1.91)
Psychological development disorder
1.53 (1.38, 1.71)
Depressive disorder
1.72 (1.55, 1.91)
Anxiety disorder
1.63 (1.47, 1.81)
Schizophrenia and psychoses
1.71 (1.54, 1.89)
Personality disorder
1.74 (1.57, 1.93)
Organic disorder
1.73 (1.57, 1.92)
Notes: Individual models were run for each subcategory. Models were adjusted for sex, early gestation (<37 weeks), mother’s age at birth, father’s age at birth, maternal marital status at birth, SES, residential remoteness, disability and maternal mental health contact. Risk estimates are presented as hazard ratios; error bars denote 95 per cent confidence intervals.
Figure 11: Risk of children with no disability exposed to DFV having a mental health subcategory compared to non-exposed children with no disability
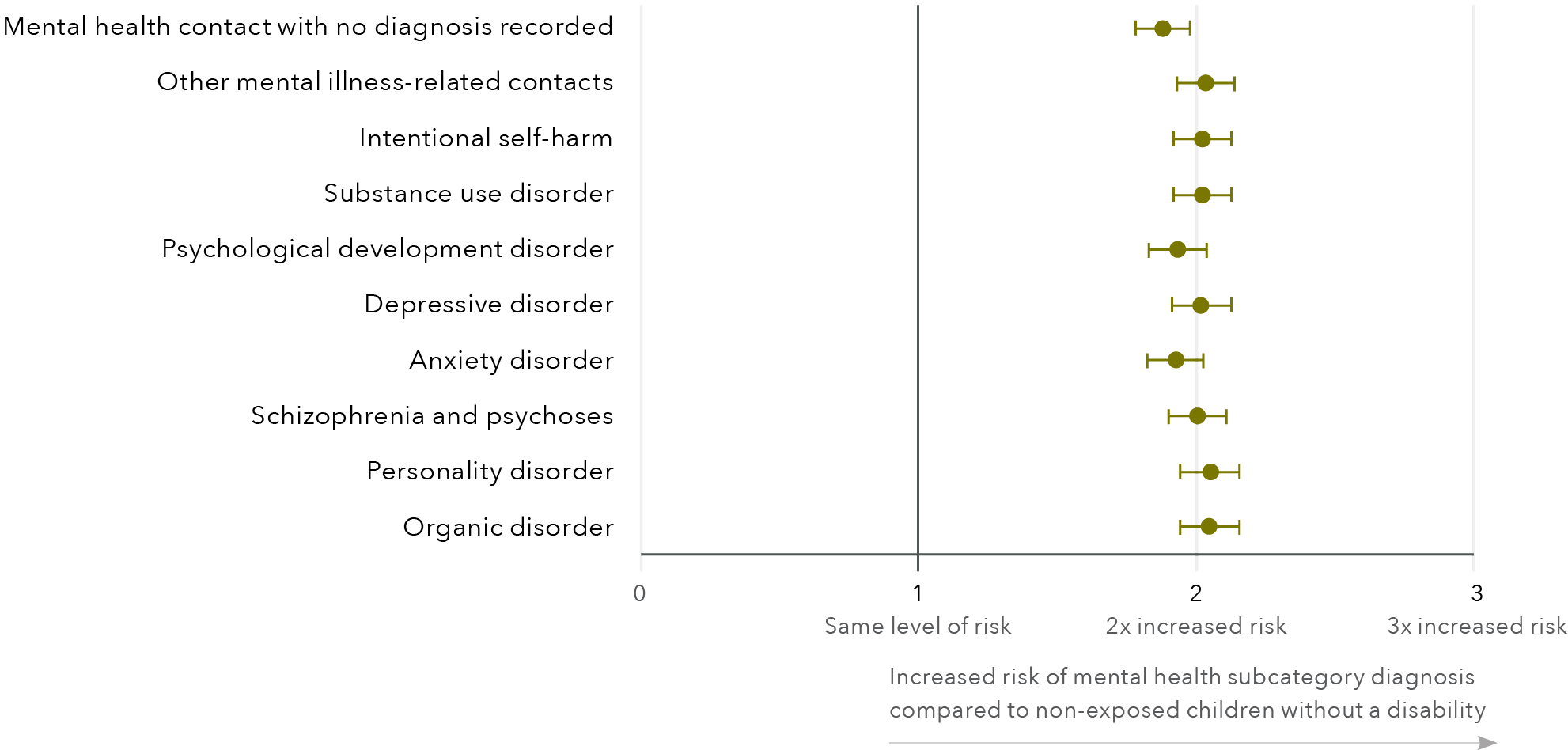
Mental health subcategory
Adjusted hazard ratios (95% CI)
Mental health contact with no diagnosis record
1.88 (1.78, 1.98)
Other mental illness-related contacts
2.03 (1.93, 2.14)
Intentional self-harm
2.02 (1.92, 2.13)
Substance use disorder
2.02 (1.92, 2.13)
Psychological development disorder
1.93 (1.83, 2.04)
Depressive disorder
2.02 (1.91, 2.12)
Anxiety disorder
1.92 (1.82, 2.03)
Schizophrenia and psychoses
2.00 (1.90, 2.11)
Personality disorder
2.05 (1.94, 2.16)
Organic disorder
2.05 (1.94, 2.16)
Notes: Individual models were run for each subcategory. Models were adjusted for sex, early gestation (<37 weeks), mother’s age at birth, father’s age at birth, maternal marital status at birth, SES, residential remoteness, disability and maternal mental health contact. Risk estimates are presented as hazard ratios; error bars denote 95 per cent confidence intervals.
Discussion
The aim of this research was to investigate the mental health service use of children exposed to DFV and the diagnosis subtypes of these children. We also aimed to identify sociodemographic characteristics that were predictive of diagnosis in children exposed to DFV. Additionally, we aimed to investigate the mental health service use and diagnosis of Aboriginal and Torres Strait Islander children and children with disability.
Mental health service contact
Findings from this research have shown that exposure to DFV in childhood is associated with an increased risk of mental health service contact during childhood. Our findings have some accord with existing research that acknowledges higher rates of DFV exposure in children using mental health services (Hultmann & Broberg, 2016; Ormhaug et al., 2012; Olaya et al., 2010). Hultmann and Broberg (2016) found that almost half of the children involved in Swedish mental health services had been exposed to DFV – five times higher than the rate of DFV in the general population. Our findings are different in that we measured mental health service contact in a DFV-exposed population and not DFV in a mental health service user population. Despite the differences, we have provided further robust evidence that DFV exposure is associated with an impact on children’s mental health.
The child’s involvement in mental health services should not necessarily be seen as a negative. Children exposed to DFV have experienced trauma and many are likely to need mental health services to aid them with addressing the trauma. However, it is concerning that, while the average age of exposure recorded in our data was 6.5 years, mental health service contact did not occur until the child was an average age of 12.5, similar to the service contact age in non-exposed children. Previous research has found that children exposed to trauma including DFV are more likely to need urgent mental health service access than those who have had no trauma exposure (Marshall et al., 2020). Early access to mental health services is important for children as it can reduce the long-term impact of mental illness (Colizzi et al., 2020; MacDonald et al., 2018). It is acknowledged that there are significant gaps in Australian mental health services for children aged0 to 12 (Australian Government, 2021), with psychiatric experts describing Australia’s mental health system as “broken” (National Mental Health Commission, 2020a). At present Australia’s mental health service is focused on specialist intervention not prevention and early intervention (Australian Government, 2021). However, the recently published National Children’s Mental Health and Wellbeing Strategy (Australian Government, 2021) aims to address these issues with priority given to children 0 to
12 years.
Early intervention is needed. This intervention should be underpinned by a public health approach addressing primary, secondary and tertiary prevention (Dahlberg & Krug, 2002; García-Moreno et al., 2015; Harvey et al., 2007). Investment is needed in primary prevention, that is, to prevent exposure before it occurs and hence eliminate subsequent negative outcomes. However, dual investment is needed in secondary and tertiary response and prevention measures to support the mental health of children exposed to DFV (National Mental Health Commission, 2020b). Early intervention for children’s mental health should address the impact of DFV exposure and its social determinants (Australian Government, 2021). This approach aligns with the National Children’s Mental Health and Wellbeing Strategy (Australian Government, 2021), which acknowledges the need to address the impact of trauma and socialdeterminants on children’s mental health and wellbeing. Without early intervention the child may potentially live with trauma and mental illness for many years impacting their ability to meet their full potential in education, relationships, employment and earning potential in adulthood (Altszuler et al., 2016; Australian Government, 2021; Clark et al., 2017; Colman et al., 2009; Erskine et al., 2016; McLeod & Kaiser, 2004). Additionally, it costs significantly more to treat mental illness in adolescence and adulthood than it does to intervene in early childhood (Teager et al., 2019). A further complexity is that the utilisation of health services for children exposed to DFV is multifaceted (Olaya et al., 2010; Onyskiw, 2002). Parents may not engage their child in mental health services for various reasons including fear of DFV being divulged by the child that may result in negative repercussions for mother and child from the perpetrator (Alaggia et al., 2011;Evans & Feder, 2016): mothers may be fearful of child removal if child protection services become involved (Alaggia et al., 2011; O’Donnell et al., 2015) and of the impact on the mother’s visa status if they are a dependant on their partner’s residency visa (Borges Jelinic, 2019). Additionally, there could be a delay due to the “sleeper effect” where symptoms may not manifest for many years after the exposure (Vu et al., 2016).
Diagnosis types
It is evident from our findings that exposure to DFV is associated with a significant impact on children’s mental health. This finding is in keeping with Bronfenbrenner’s (1977) theory that a child’s environment impacts human development. Children exposed to DFV were statistically more likely to have a higher risk in eight of the 10 mental health diagnosis subcategories than non-exposed children. The highest associated risk observed was a two-fold increased risk in substance use disorder. Our finding has some accord with previous longitudinal research that reported exposure to adverse childhood experiences, including DFV, was predictive of substance misuse (Rogers et al., 2021). Rogers and colleagues (2021) investigated substance misuse in children and young people from 14 to 26 years of age, finding that it increased at higher rates over time into early adulthood for children exposed to adverse events compared to those not exposed. The mental healthof our cohort was investigated until they reached 18 years of age. In light of the findings by Rogers and colleagues (2021) there is a need to investigate the mental health of children past childhood and into adulthood. For women subjected to DFV it is acknowledged that many misuse substances as a coping mechanism (Gezinski et al., 2021). For some children exposed to DFV substance use may also be a coping mechanism; further research is needed to gain a greater understanding of substance use in children exposed to DFV.
We also found an increased risk of personality disorder to be associated with DFV exposure. Personality disorders are thought to be caused by a combination of genetic and environmental factors, including trauma (Cattane et al., 2017). Our finding aligns with the cross-sectional research of Afifi and colleagues (2019) who found maltreatment in childhood, including DFV, was associated with an increased likelihood of personality disorder. Previous research has found a clear relationship between personality disorder and DFV perpetration and victimisation (Collison & Lynam, 2021; Jackson et al., 2015). Additionally, in some cases, children exposed to DFV may be at risk of becoming perpetrators or victims of DFV in adulthood (Ehrensaft et al., 2003; Smith et al., 2011). For the children exposed to DFV with personality disorder, it could be postulated that the risk of transgenerational abuse may be greater. The evidence, however, is not robust and, assuch, further research is clearly warranted to understand these complex associations more fully.
Exposure to DFV was associated with a 49 per cent increased risk of anxiety disorder, when compared to non-exposed children. While our findings align with recent Australian research (Gartland et al., 2021), some differences are noted. Gartland and colleagues (2021) reported a twofold increased likelihood of anxiety in children who were recently exposed to DFV which differs from our reported increase. The differences may be attributed to the approach used to identify anxiety and the differing ages between the studies. Gartland and colleagues measured anxiety at age 10, whereas the children’s anxiety in our cohort could be identified at any point in childhood. The key point, however, is that the children identified in our data as having their first mental health contact were, on average, aged 12.5 years, and therefore missing early childhood intervention. In consideration of Gartland’s findings and the Australian Government’s (2021) acknowledgement thatthere are service gaps in Australian mental health services for children aged 0 to 12 it is likely that our measurement of risk is an underestimation of the true association.
In keeping with existing literature (Huang et al., 2021; Kennedy et al., 2010; Kimball, 2016) we found that children’s exposure to DFV was associated with an increased risk of depression compared to non-exposed children. The aetiology of depression is multifactorial, with multiple ecological factors thought to play a part including genetics, exposure to stressful events (including DFV exposure) and low SES (Colman & Ataullahjan, 2010; Najman et al., 2010; Zalsman et al., 2006). As an example of the impact of low SES, recent international research (Marçal, 2021) has reported that housing insecurity mediates the risk of depression in children exposed to DFV. In Australia, utilising data from the Australian Specialist Homelessness Services Collection (AIHW, 2021c) would allow for the investigation of housing insecurity as a mediator of depression, and other outcomes, from an Australian perspective. A further advantage is that it would provide anotheravenue to identify DFV exposure as 42 per cent of clients seeking assistance from specialist homelessness services in Western Australia did so due to DFV (AIHW, 2019).
We found that, compared to non-exposed children, children exposed to DFV had a 52 per cent increased risk of having a mental health contact with no diagnosis recorded. This category captured children who were in MHIS data but had no diagnosis or had a mental health diagnosis in HMDC data or EDDC data. It is not clear from the data why this is the case; it may be for multiple reasons. The child may not engage in services to enable a diagnosis by clinicians. Additionally, the clinicians may be unaware of the DFV which prevents a full understanding of the child’s environment impacting clinical diagnosis. As discussed previously the lack of classification for developmental trauma may result in an absence of diagnosis so the child may not receive appropriate support and care. Further investigation is needed to gain an understanding of potential barriers in the support and treatment of children exposed to DFV.
The focus on diagnosis is highlighted in the National Children’s Mental Health and Wellbeing Strategy (Australian Government, 2021). The strategy proposes a cultural shift in the way that we think about the mental health and wellbeing of children – that is, a greater focus on a child’s functioning rather than diagnosis. The strategy argues that funded services should be available for children at the point that they begin to struggle, rather than delaying services until the child is unwell and is given a diagnosis. The strategy highlighted that this approach aligned with the Aboriginal and Torres Strait Islander concept of emotional wellbeing.
Predictive characteristics for mental health service contact
Overall, the characteristics that increased the risk of mental health service contact for children exposed to DFV were similar to those of non-exposed children. However, significant differences were noted in maternal age and mother’s mental health contact. For children exposed to DFV being born to a mother aged under 30 was associated with a reduced risk of mental health service contact. This reduction was not observed in the non-exposed children. Additionally, having a mother with a mental health service contact was associated with a 34 per cent increased risk of mental health service contact for non-exposed children, but it did not increase the risk for children exposed to DFV. It is not clear from our data why this is the case. Our findings are in contrast to existing literature that found parental mental illness can increase the risk of mental illness for the child (Matijasevich et al., 2014; Reupert et al., 2013). However, it is accepted that thecombination of DFV and maternal mental illness can disrupt parenting (Greene et al., 2018) which may reduce engagement in services for the child. Previous research has acknowledged the relationship between DFV and women’s mental health is complex and bidirectional in nature, with both highly associated with each other (Mason & O’Rinn, 2014). This may make the association of maternal mental illness and children’s mental illness harder to disentangle for families subjected to DFV. It should be noted that the reduction in risk for children exposed to DFV does not indicate that maternal mental illness or being born to a mother under 30 years are protective factors for mental health issues. Rather, these associations should be viewed as potential barriers that require further exploration.
Existing research is equivocal on whether sex impacts the mental health of children exposed to DFV (e.g. Sternberg et al., 2006). We found that, overall, sex had no impact on the risk of mental health service contact for children exposed to DFV. However, we did find differences in service use over time. Females exposed to DFV had lower probability of mental health service contact than their male counterparts between the age of 7 to 14. However, by the age of 15 years the probability of mental health service contact was similar for males and females. Our findings highlight the importance of investigating mental health service outcomes over an extended period. Without longitudinal research the association of characteristics on mental health for those exposed to DFV may be misinterpreted, impacting the ability to appropriately target services.
Differences in the sexes were noted in specific diagnosis subtypes. Being female increased the risk of personality disorder category in children exposed to DFV by 100 per cent and by 48 per cent in non-exposed children. Conversely, in the other mental illness-related contacts category higher risk was seen in non-exposed females who had a 291 per cent increased risk whereas exposed female children had a 100 per cent increased risk. Exposure to trauma in childhood is thought to increase the risk of personality disorder (Porter et al., 2020; Sher et al., 2015). The association of sex with personality disorders is complex, and findings from existing research are equivocal (Schulte Holthausen & Habel, 2018). One reason for the inconsistency is thought to be the influence of gender stereotypes on clinicians’ diagnosis of certain personality disorders (Crosby & Sprock, 2004; Schulte Holthausen & Habel, 2018). The higher risk of personalitydisorder seen in exposed females needs further investigation. It may be that there is greater bias in the diagnosis of personality disorder in females exposed to DFV due to gender stereotypes, or there may be some physiological underpinnings.
The findings on predictive characteristics support the proposal of ecological theory (Bronfenbrenner, 1977) that multiple variables influence a child’s mental health (D’Andrea & Graham-Bermann, 2017). Importantly, not all children with highlighted characteristics, such as a mother with mental illness or those who were born to a mother under 30 years, had a mental health contact or mental health diagnosis. This supports the theory (Bronfenbrenner & Morris, 2007) that developmental processes are probabilistic, not deterministic.
Aboriginal and Torres Strait
Islander children
Aboriginal and Torres Strait Islander children were overrepresented in our cohort with 62 per cent of children exposed to DFV being Aboriginal and Torres Strait Islander. This overrepresentation may be explained, in part, by high rates of DFV experienced by Aboriginal and Torres Strait Islander women, including mothers (ABS, 2016b; Orr, Preen et al., 2019). A further explanation for overrepresentation may be the source of our DFV identification: police and hospital data. Some studies suggest that the likelihood of being charged for DFV is increased by a variety of socioeconomic and demographic characteristics, such as Aboriginal status (Cunneen, 2010; Jeffries & Bond, 2015). Studies also show that Aboriginal and Torres Strait Islander women are more likely to be hospitalised for DFV than non-Aboriginal and Torres Strait Islander women (AIHW, 2006; Orr, Preen et al., 2019). DFV is not consistent with traditional Aboriginal and Torres Strait Islanderculture and the overrepresentation of Aboriginal and Torres Strait Islander children in this study should be understood in the context of the multiple disadvantages faced by Aboriginal and Torres Strait Islander peoples as a result of colonisation and not as an indicator of a racial determinant (Blagg et al., 2020; Our Watch, 2018). Additionally, Aboriginal and Torres Strait Islander women and children may be experiencing DFV perpetrated by non-Aboriginal and Torres Strait Islander people.
Similar to the full cohort, we found that for Aboriginal and Torres Strait Islander children who were exposed to DFV, having a mother with a mental health service contact reduced the risk of mental health service contact for the child. This was in contrast to the non-exposed children where an increase in service contact was noted. Findings from the Western Australian Aboriginal Child Health Survey (Zubrick et al., 2005) highlighted that Aboriginal children whose primary carer had used mental health services were more likely to have a mental health service use than those with a carer who had not used mental health services. However, the survey findings did not account for DFV exposure. Given the differences in mental health contact between children exposed to DFV and non-exposed children and the high rates of DFV in Aboriginal communities, future research investigating the mental health of Aboriginal and Torres StraitIslander children should consider the impact of
DFV exposure.
Our findings suggest that co-occurring DFV and maternal mental illness is a barrier to mental health service use for children exposed to DFV. A potential explanation may be that Aboriginal and Torres Strait Islander families experiencing multiple issues such as DFV and maternal and child mental illness are wary of service engagement due to fear of child removal (O’Donnell et al., 2015).
Both Aboriginal and Torres Strait Islander children exposed and not exposed to DFV had an increased risk of mental health service contact if they lived in a major city. This increase was not consistent with the full cohort where being from a major city had no impact on the risk of mental health service contact for both exposed and non-exposed children. Additionally, for Aboriginal and Torres Strait Islander children not exposed to DFV, living in a very remote location decreased their risk of mental health service contact by 16 per cent. However, for children exposed to DFV, being from a very remote area had no impact on the risk of mental health service contact. These findings cannot be taken to mean that children exposed to DFV out of the metropolitan area do not have as high a risk of mental illness – instead it may be due to the greater challenges in accessing mental health services outside the metropolitan area (National Mental Health Commission,2018). Previous research (Cassells et al., 2014) has reported that the lack of culturally appropriate mental health services for Aboriginal and Torres Strait Islander children living in remote and isolated communities is a barrier to accessing and engaging in services. Our findings have implications for regional and remote resource needs and mental health service provision to support children exposed to DFV. The newly launched Aboriginal Empowerment Strategy – Western Australia 2021–2029 (Government of Western Australia, 2021b) acknowledged the need for place-based partnership engagement. To ensure culturally responsive and secure services, services should be tailored to specific geographic areas to match local priorities and contexts, all while keeping Aboriginal culture at the forefront (Government of Western Australia, 2021b).
For Aboriginal and Torres Strait Islander children, exposure to DFV was associated with a significantly increased risk of intentional self-harm, which was not seen in non-exposed Aboriginal and Torres Strait Islander children but aligns with previous Australian research (Leckning et al., 2020). Self-harm is a major public health issue and is the leading cause of death in Australian children aged 5 to 17 (ABS, 2021b). The higher rates of intentional self-harm seen in Aboriginal and Torres Strait Islander children exposed to DFV have been attributed to the effects of intergenerational trauma stemming from the impacts of colonisation and Stolen Generation policies on family and community functioning (Dudgeon et al., 2017; Leckning et al., 2020). In addressing the high rates of intentional self-harm for Aboriginal and Torres Strait Islander children, the renewed Closing the Gap campaign (Commonwealth of Australia. Department of the Prime Minister andCabinet, 2021) recognises the need for strategies to promote high levels of social and emotional wellbeing. For some Aboriginal and Torres Strait Islander children and families, mainstream, western concepts of mental health do not directly translate into the more holistic framework of social and emotional wellbeing (Leckning et al., 2019). Aboriginal and Torres Strait Islander expertise in culturally appropriate service provision is needed to lead the way forward.
Our findings highlight the importance of Closing the Gap’s Target 13 – “families and households are safe” – which aims to reduce all forms of DFV against Aboriginal and Torres Strait Islander women and children by at least 50 per cent by 2031 (Commonwealth of Australia. Department of the Prime Minister and Cabinet 2021). Characteristics such as residential remoteness and maternal mental health contact were found to impact mental health service use and diagnosis in Aboriginal and Torres Strait Islander children, and these characteristics are worthy of further research. Aboriginal and Torres Strait Islander communities are best positioned to identify specific research questions to better understand the impact DFV exposure has on children’s mental health in their communities.
The Fourth National Action Plan of the National Plan to Reduce Violence against Women and their Children has prioritised support for Aboriginal women who are disproportionately exposed to DFV (Council of Australian Governments, 2019). There is a need for Aboriginal and Torres Strait Islander peoples to drive the development of multidisciplinary and multi-agency approaches that are both trauma informed and culturally appropriate for Aboriginal communities. To achieve this and to improve outcomes, government and service providers need to work in partnership with
Aboriginal communities.
Children with disability
To date, the impact of DFV on children with disability is poorly understood (Dababnah et al., 2018; Robinson et al., 2020). Our findings suggest that DFV exposure may be a barrier to service access for children with disability. For children exposed to DFV, having disability was associated with a 41 per cent increased chance of having a mental health service contact – that is, less than half the risk seen in non-exposed children with disability. Children with disability face multiple barriers accessing health services in a timely manner including cost, inadequate transportation, inaccessibility of buildings and discrimination by health professionals (AIHW, 2020b; VicHealth, 2012). For children exposed to DFV, the mother may not engage the child in mental health services for fear of child removal, since children with disability are more likely to have contact with child protection services and the out-of-home care system (Commonwealth of Australia, 2015;Hindmarsh et al., 2021). Further research is needed to gain a greater understanding of DFV exposure on mental health service access.
For children with disability who were exposed to DFV, being born pre-term (prior to 37 weeks gestation) was associated with an increased risk of mental health service contact. This increase was not observed in non-exposed peers. It is not clear from the data why pre-term birth is associated with an increased risk in children exposed to DFV. While our average age of exposure was 6.5 years, it is acknowledged that DFV can occur for many years before women report it or engage in services (Graham-Bermann & Perkins, 2010; Loxton et al., 2017). Therefore, it may be that some mothers were subjected to DFV while pregnant, which increases not only the risk of pre-term birth (Alhusen et al., 2015; Lipsky et al., 2003) but subsequent mental health issues for the child (Martinez-Torteya et al., 2015). Further research is required to gain a greater understanding of the association of pre-term birth and the mental health of children exposed to DFV, including thecapture of DFV in pregnancy.
Strengths and limitations
Strengths
The main strength of the research was the use of population level administrative data, linked across multiple agencies, at both the child and parent level to investigate the mental health of children exposed to DFV. The use of linked police and hospital data to identify DFV exposure enabled investigations of high-risk groups not captured in previous mental health research. Researching DFV is a complex task. The intimate context of the phenomenon means the act is not observed and, in many cases, is unreported (Phillips & Vandenbroek, 2014). The stigma related to the issue and the safety risk to the mothers and children also account for a high rate of non-responses within existing DFV research (Ruiz-Pérez et al., 2007). Identifying and researching children’s exposure to DFV is further complicated by maternal fear that their child may be removed if they disclose (Wilson et al., 2017). Due to these complexities, research related to childrenexposed to DFV is predominately based on small samples of children involved in specialist services, representing a subsection of those exposed. The use of the Western Australian Data Linkage System ensured that ethical and privacy standards were upheld and facilitated the ability to identify DFV and outcomes of a hidden population. The availability of dates of DFV events and outcome events allowed longitudinal follow-up. Additionally, the linked population data provided a wealth of information on multiple ecological factors at the child, parent and community level, enabling multivariate analysis when investigating the mental health of children exposed to DFV. The use of linked administrative data eliminated recall bias, reporting bias and loss-to-follow-up seen in existing literature.
As we had no information on the lived experiences of the children or families included in the study, our research was further strengthened by the community and consumer reference groups who aided interpretation of the findings.
Limitations
While the use of linked administrative data provides many advantages, there are some limitations that should be noted. While most violence against women is perpetrated by a current or former male intimate partner, it should be acknowledged that the DFV in some cases identified in the hospital data may have been perpetrated by someone other than a male intimate partner. DFV classification in hospital data is overly complex and needs to be streamlined to better capture the experiences of women.
Aboriginal and Torres Strait Islander children were overrepresented in our research cohort. This could be, in part, due to the police records of DFV requiring a charge to be made against the man; there is evidence to suggest that the likelihood of being charged for DFV is increased by a variety of socioeconomic and demographic characteristics, such as Aboriginal status (Australian Law Reform Commission, 2018; Cunneen, 2010; Jeffries & Bond, 2015). Despite a call-out occurring, on average, every 10 minutes in Western Australia for DFV, our exposed cohort comprised 5,736 mothers over five years. This equates to the number of call-outs police receive in 40 days. Therefore, our data are an underestimation of DFV and not generalisable to women who are victims of DFV where a man is not charged with an offence.
The children identified as exposed to DFV in this report were only recognised because of the mother’s involvement in police or hospital services. As such, the data may be subject to selection bias, capturing mainly the more physical cases of DFV, and may underestimate the impact of DFV exposure on children’s mental health outcomes due to the fact that not all children exposed to DFV were captured. It is therefore likely that the estimates presented in this report are conservative estimates of the association between DFV and the mental health of children exposed to DFV. Furthermore, it was assumed that the children exposed to DFV resided with their mother, but this may not be the case for all children captured.
Additionally, while rich data are made available from administrative datasets, the datasets provided no or limited data in relation to family functioning, family structure and social support. As such, there are likely to be a number of unmeasured characteristics that would have influenced outcomes for the child.
While the identification of disability was based on categories used in previous research (Maclean, Sims et al., 2017), the capture of disability is limited. Individuals differ on how they define their disability status and our definition does not take into account the complex and multidimensional nature of disability. Also, our definition is limited in its scope as it does not capture chronic health conditions such as asthma, epilepsy or permanent injuries which some of the literature incudes in its disability categories.
Our capture of mental illness in children was identified by public and private hospitalisations and ED attendance, and public outpatient mental health services. Many children with mental illness will not be identified in these data. The most recent Australian Child and Adolescent Survey of Mental Health and Wellbeing (Lawrence et al., 2015, p. 6) highlighted that only 6 per cent of children (4 to 17 years) with a mental health disorder had attended hospital or an emergency department for their mental health in the past 12 months. Furthermore, the survey highlighted that only 3 per cent of children (4 to 17 years) with mental illness had attended outpatient mental health services in the previous 12 months (Lawrence et al, 2015, p. 6). However, the survey found that 42 per cent of children had seen their GP for mental illness in the previous 12 months. Therefore, our identification of service use and diagnosis for childrenexposed to DFV is underestimated. Additionally, the findings of our results may not reflect those of children who have mental illness and use other services.
Distribution of categories within the cohort demographic characteristics varied. However, this was accounted for in the multivariable analysis employed from which the findings are reported. Finally, as an observational study, the results of the research contained in this report highlight an association, and do not indicate causality between DFV exposure and the development of mental illness.
Directions for future research
This report highlighted that there is a substantial period of time between children’s exposure to DFV and their contact with mental health services. Early access to mental health services is important for children as it can reduce the long-term impact of mental illness (MacDonald et al., 2018). It is imperative to ensure improved mental health outcomes for children exposed to DFV that research to understand factors associated with delay in service contact is undertaken as a priority. It is equally imperative that the results provide evidence to ensure the availability of adequate and appropriate services which can be accessed in a timely manner.
This report details the mental health service use and diagnosis of children exposed to DFV. It is acknowledged that children with mental health issues are more likely to have mental health issues in adulthood (Kessler, 2005; Ravens-Sieberer et al., 2015). Future research is needed to investigate the mental health of the children exposed to DFV into their adulthood. Additionally, further research is needed on the transition of care, for children exposed to DFV, from children’s mental health services to adult services. This transition period is often poorly managed (Crowley et al., 2011) with continuity of care disruption increasing disengagement from services (Singh, 2009). As young people with complex needs are at greater risk of “falling thorough the gaps” in care transition (Singh, 2009), attention to those exposed to DFV is needed.
Further research is required utilising multiple sources of linked data to identify both DFV and mental illness. Data sources such as the Australian Specialist Homelessness Services Collection (AIHW, 2021c), primary care general practice data, prescription data, school nurse data and private mental health outpatient services are required to gain a greater understanding of the effects of exposure to DFV on children’s mental health. The linked data should be complemented by combining data from population-based surveys, longitudinal surveys and social indicators (Hertzman & Williams, 2009). This multiple source approach would largely overcome the limitations of using each source separately and benefit from the strengths of each.
There is a need for research driven by Aboriginal and Torres Strait Islander peoples on the mental health of Aboriginal and Torres Strait Islander children given their disproportionate exposure to DFV. The findings contained in this report have the potential to be a stepping stone from which a holistic, culturally appropriate program of research can be developed.
We were unable to investigate the mental health service use of children born to CALD parents. Given that Australia continues to settle immigrants and those fleeing persecution and violence, having insufficient data available to undertake robust research to understand mental health outcomes and appropriate interventions in these populations is worrying. Ensuring that government and not-for-profit agencies routinely collect this data and make it available for research purposes is pivotal in enabling the urgently needed research.
Implications for policy and practice
Our research has shown that DFV exposure is associated with an increased risk of mental health service contact and diagnosis of mental illness. Early intervention is required. Many children exposed to DFV are not engaged in mental health services until years after the exposure. Our findings provide further support for the National Children’s Mental Health and Wellbeing Strategy (Australian Government, 2021) in that funded services should be available for children at the point that they begin to struggle, rather than services being delayed until the child is unwell and given a diagnosis. Our findings also add further support for the need for a dedicated standalone national response and matching actions strategy for the mental health of children exposed to DFV (Australian Government, 2021).
Children exposed to DFV often live with complex issues such as maternal mental illness and disability. Services to support children exposed to DFV must be well resourced and holistically focused with collaborative, multidisciplinary teams and cross-agency collaboration that provides continuity of care for children and their families with multiple and complex issues.
It is important that mental health clinicians are aware of trauma, including DFV exposure, during childhood. Clinicians need to have knowledge of DFV and its implications for mental health as well as the ability to appropriately and safely respond to children exposed to DFV (McTavish et al., 2016). These skills need to be taught to clinicians during their training and offered as ongoing professional development to enable clinicians to stay abreast of contemporary developments. At present DFV training is not part of the mandatory suite of training across Western Australian health services. A national approach should be taken to ensure that all registered and non-registered staff within public, private and NGO health services are provided with DFV training.
Aboriginal and Torres Strait Islander peoples should be provided with the opportunity and resources to develop policies and programs to support Aboriginal and Torres Strait Islander children who experience exposure to DFV.
Children and their families subjected to DFV are in contact with multiple agencies that may include education, health, police and child protection, and each agency provides a potential point of intervention. As such, it is imperative that these agencies, along with children’s mental health services, are embedded in, and part of, a broader collaborative, multiagency and multidisciplinary response to DFV; they need to be adapted to “fit” with the existing local response to DFV and to avoid unwarranted duplication of services.
To support service engagement and reduce the re-traumatisation of children exposed to DFV, service responses must be trauma informed and culturally responsive and secure.
Exposure to DFV is associated with an increased risk of mental health disorders in children. Our findings highlight the importance of the continuation of collective prevention efforts nationally and in each jurisdiction to reduce and eradicate DFV.
Conclusion
This study was undertaken to gain an understanding of the mental health service contact and diagnosis categories of children exposed to DFV. Using linked administrative data has enabled us to investigate a population that is often hidden. Children’s exposure to DFV is associated with an increased risk of mental health service use and mental health diagnosis in childhood. There are sociodemographic characteristics that appear to be factors associated with children exposed to DFV accessing mental health services including being born to a mother under 30 and a mother with mental illness. Additionally, many children are not accessing mental health services until several years after their exposure. These findings highlight the need for targeted government funding for early intervention mental health services for children exposed to DFV. Intervention strategies should be underpinned by a public health approach and include multidisciplinary, multi-agencyapproaches that are trauma-informed. Aboriginal and Torres Strait Islander children are overrepresented in our exposed cohort. This provides further evidence for the need to have culturally appropriate services led by and tailored for Aboriginal and Torres Strait Islander peoples.
References
Abel, K. M., Hope, H., Swift, E., Parisi, R., Ashcroft, D. M., Kosidou, K., Osam, C. S., Dalman, C., & Pierce, M. (2019). Prevalence of maternal mental illness among children and adolescents in the UK between 2005 and 2017: A national retrospective cohort analysis. Lancet Public Health, 4(6), e291–e300. https://doi.org/10.1016/S2468-2667(19)30059-3
Abrams, Z. (2021). Improved treatment for developmental trauma. American Psychological Association, 52(5), 38. https://www.apa.org/monitor/2021/07/ce-corner-developmental-trauma
Achenbach, T. (1991). Manual for the Child Behavior Checklist/4–18 and 1991 profile. University of Vermont Department of Psychiatry.
Afifi, T. O., Fortier, J., Sareen, J., & Taillieu, T. (2019). Associations of harsh physical punishment and child maltreatment in childhood with antisocial behaviors in adulthood. JAMA Network Open, 2(1), e187374. https://doi.org/10.1001/jamanetworkopen.2018.7374
Al-Yaman, F. (2017). The Australian Burden of Disease Study: Impact and causes of illness and death in Aboriginal and Torres Strait Islander people, 2011. Public Health Research & Practice, 27(4). https://doi.org/10.17061/phrp2741732
Alaggia, R., Regehr, C., & Jenney, A. (2012). Risky business: An ecological analysis of intimate partner violence disclosure. Research on Social Work Practice, 22(3), 301–312. https://doi.org/10.1177/1049731511425503
Alhusen, J. L., Ray, E., Sharps, P., & Bullock, L. (2015). Intimate partner violence during pregnancy: Maternal and neonatal outcomes. Journal of Women’s Health, 24(1), 100–106. https://doi.org/10.1089/jwh.2014.4872
Altszuler, A. R., Page, T. F., Gnagy, E. M., Coxe, S., Arrieta, A., Molina, B. S. G., & Pelham, W. E. (2016). Financial dependence of young adults with childhood ADHD. Journal of Abnormal Child Psychology, 44, 1217–1229. https://doi.org/10.1007/s10802-015-0093-9
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). American Psychiatric Association.
Anderson, D. M., Cesur, R., & Tekin, E. (2015). Youth depression and future criminal behavior. Economic Inquiry, 53(1), 294–317. https://doi.org/10.1111/ecin.12145
Antle, B., Barbee, A., Yankeelov, P., & Bledsoe, L. (2010). A qualitative evaluation of the effects of mandatory reporting of domestic violence on victims and their children. Journal of Family Social Work, 13, 56–73. https://doi.org/10.1080/10522150903468065
Australian Bureau of Statistics. (2011a). Australian and New Zealand Standard Offence Classification (ANZSOC), 2011. https://www.abs.gov.au/ausstats/[email protected]/mf/1234.0
Australian Bureau of Statistics. (2011b). 2006 Remoteness area from 2006 collection districts correspondence. https://www.abs.gov.au/ausstats/[email protected]/Products/1216.0.15.003~2006~Main+Features~2006+RA+from+2006+CD+Correspondence?OpenDocument
Australian Bureau of Statistics. (2016a). Disability, Ageing and Carers, Australia: Summary of findings, 2015 (ABS cat. no. 4430.0). https://www.abs.gov.au/ausstats/[email protected]/Lookup/4430.0main+features202015
Australian Bureau of Statistics. (2016b). National Aboriginal and Torres Strait Islander Social Survey 2014–15 (ABS cat. no. 4714.0). https://www.abs.gov.au/AUSSTATS/[email protected]/DetailsPage/4714.02014-15?OpenDocument
Australian Bureau of Statistics. (2017a). Personal Safety Survey 2016 (ABS cat. no. 4906.0). ABS.
Australian Bureau of Statistics. (2017b). 2016 Census QuickStats. https://quickstats.censusdata.abs.gov.au/census_services/getproduct/census/2016/quickstat/5?opendocument
Australian Bureau of Statistics. (2017c). Australian Demographic Statistics, December 2016. https://www.abs.gov.au/AUSSTATS/[email protected]/DetailsPage/3101.0Dec%202016?OpenDocument
Australian Bureau of Statistics. (2017d). Census of Population and Housing – Counts of Aboriginal and Torres Strait Islander Australians. https://www.abs.gov.au/statistics/people/aboriginal-and-torres-strait-islander-peoples/census-population-and-housing-counts-aboriginal-and-torres-strait-islander-australians/latest-release
Australian Bureau of Statistics. (2018a). Socio-economic indexes for areas. https://www.abs.gov.au/websitedbs/censushome.nsf/home/seifa
Australian Bureau of Statistics. (2018b). The Australian statistical geography standard (ASGS) remoteness structure. https://www.abs.gov.au/websitedbs/D3310114.nsf/home/remoteness+structure
Australian Bureau of Statistics. (2018c). Estimates of Aboriginal and Torres Strait Islander Australians. https://www.abs.gov.au/statistics/people/aboriginal-and-torres-strait-islander-peoples/estimates-aboriginal-and-torres-strait-islander-australians/latest-release#data-download
Australian Bureau of Statistics. (2019). Disability, Ageing and Carers, Australia: Summary of findings. https://www.abs.gov.au/statistics/health/disability/disability-ageing-and-carers-australia-summary-findings/latest-release#children-with-disability
Australian Bureau of Statistics. (2021a). 2016 Census QuickStats. https://quickstats.censusdata.abs.gov.au/census_services/getproduct/census/2016/quickstat/5?opendocument
Australian Bureau of Statistics. (2021b). Causes of death, Australia. https://www.abs.gov.au/statistics/health/causes-death/causes-death-australia/latest-release#intentional-self-harm-deaths-suicide-in-australia
Australian Early Development Census. (2022). About the AEDC data. https://www.aedc.gov.au/researchers/about-the-aedc-data
Australian Government. (2018). Data integration: Roles and responsibilities of data custodians. https://toolkit.data.gov.au/Data_Integration_-_Roles_and_responsibilities_of_data_custodians.html
Australian Government. (2021). National Children’s Mental Health and Wellbeing Strategy. https://www.mentalhealthcommission.gov.au/getmedia/e369a330-f8c3-4b9e-ab76-7a428f9ff0e3/national-childrens-mental-health-and-wellbeing-strategy-report-25oct2021
Australian Human Rights Commission. (2015). Face the facts: Aboriginal and Torres Strait Islander peoples. https://www.humanrights.gov.au/our-work/education/face-facts-aboriginal-and-torres-strait-islander-peoples
Australian Human Rights Commission. (2018). Information relating to Australia’s joint fifth and sixth report under the Convention on the Rights of the Child, second report on the Optional Protocol on the sale of children, child prostitution and child pornography, and second report on the Optional Protocol on the involvement of children in armed conflict. https://www.humanrights.gov.au/our-work/childrens-rights/publications/report-un-committee-rights-child-2018
Australian Institute of Family Studies. (2018). What is child abuse and neglect? https://aifs.gov.au/cfca/publications/what-child-abuse-and-neglect
Australian Institute of Health and Welfare. (2006). Family violence among Aboriginal and Torres Strait Islander peoples. https://www.aihw.gov.au/reports/indigenous-australians/family-violence-indigenous-peoples/contents/table-of-contents
Australian Institute of Health and Welfare. (2018a). Culturally and linguistically diverse populations. https://www.aihw.gov.au/getmedia/f3ba8e92-afb3-46d6-b64c-ebfc9c1f945d/aihw-aus-221-chapter-5-3.pdf.aspx
Australian Institute of Health and Welfare. (2018b). Family, domestic and sexual violence in Australia, 2018. https://www.aihw.gov.au/reports/domestic-violence/family-domestic-sexual-violence-in-australia-2018/contents/table-of-contents
Australian Institute of Health and Welfare. (2018c). Aboriginal and Torres Strait Islander adolescent and youth health and wellbeing 2018. https://www.aihw.gov.au/reports/indigenous-australians/atsi-adolescent-youth-health-wellbeing-2018/contents/summary
Australian Institute of Health and Welfare. (2019). Family, domestic and sexual violence in Australia: Continuing the national story. https://www.aihw.gov.au/getmedia/b0037b2d-a651-4abf-9f7b-00a85e3de528/aihw-fdv3-FDSV-in-Australia-2019.pdf.aspx?inline=true
Australian Institute of Health and Welfare. (2020a). Australia’s children: Chronic conditions and burden of disease. https://www.aihw.gov.au/reports/children-youth/australias-children/contents/health/chronic-conditions
Australian Institute of Health and Welfare. (2020b). People with disability in Australia. https://www.aihw.gov.au/reports/disability/people-with-disability-in-australia/contents/summary
Australian Institute of Health and Welfare. (2021a). Mental health services in Australia. https://www.aihw.gov.au/reports/mental-health-services/mental-health-services-in-australia/report-contents/expenditure-on-mental-health-related-services
Australian Institute of Health and Welfare. (2021b). Child protection Australia. https://www.aihw.gov.au/getmedia/c3b0e267-bd63-4b91-9ea6-9fa4d14c688c/aihw-cws-78.pdf.aspx?inline=true
Australian Institute of Health and Welfare. (2021c). Specialist Homelessness Services Collection. https://www.aihw.gov.au/about-our-data/our-data-collections/specialist-homelessness-services-collection
Australian Law Reform Commission. (2018). Pathways to justice: Inquiry into the incarceration rate of Aboriginal and Torres Strait Islander peoples (ALRC Report 133). https://www.alrc.gov.au/publication/pathways-to-justice-inquiry-into-the-incarceration-rate-of-aboriginal-and-torres-strait-islander-peoples-alrc-report-133/14-police-accountability/background-34/
Australia’s National Research Organisation for Women’s Safety. (2020a). Improving family violence legal and support services for Aboriginal and Torres Strait Islander peoples: Key findings and future directions (Research to policy and practice, 25–26/2020). ANROWS.
Australia’s National Research Organisation for Women’s Safety. (2020b). Australia’s National Research Agenda to Reduce Violence against Women and their Children: ANRA 2020–2022. ANROWS.
Bailey, B. A. (2010). Partner violence during pregnancy: Prevalence, effects, screening, and management. International Journal of Women’s Health, 2, 183–197. https://doi.org/10.2147/IJWH.S8632
Bair-Merritt, M., Johnson, S., Okelo, S., & Page, G. (2012). Intimate partner violence exposure, salivary cortisol, and childhood asthma. Child Abuse & Neglect, 36(7), 596–601. https://doi.org/10.1016/j.chiabu.2011.12.002
Bair-Merritt, M. H., Ghazarian, S. R., Burrell, L., Crowne, S. S., McFarlane, E., & Duggan, A. K. (2015). Understanding how intimate partner violence impacts school age children’s internalizing and externalizing problem behaviors: A secondary analysis of Hawaii Healthy Start Program evaluation data. Journal of Child & Adolescent Trauma, 8(4), 245–251. https://doi.org/10.1007/s40653-015-0066-8
Baldry, E., Bratel, J., & Breckenridge, J. (2006). Domestic violence and children with disabilities: Working towards enhancing social work practice. Australian Social Work, 59(2), 185–197. https://doi.org/10.1080/03124070600651895
Barker, E. D., Jaffee S. R., Uher, R., & Maughan, B. (2011). The contribution of prenatal and postnatal maternal anxiety and depression to child maladjustment. Depress Anxiety, 28, 696–702.
Bell, M. F., Bayliss, D. M., Glauert, R., & Ohan, J. L. (2018). Using linked data to investigate developmental vulnerabilities in children of convicted parents. Developmental Psychology, 54(7), 1219–1231. https://doi.org/10.1037/dev0000521
Berg, K., Bender, A., Evans, K., Holmes, M., Davis, A., Scaggs, A., & King, J. (2020). Service needs of children exposed to domestic violence: Qualitative findings from a statewide survey of domestic violence agencies. Children and Youth Services Review, 118, 105414. https://doi.org/10.1016/j.childyouth.2020.105414
Bidarra, Z. S., Lessard, G., & Dumont, A. (2016). Co-occurrence of intimate partner violence and child sexual abuse: Prevalence, risk factors and related issues. Child Abuse & Neglect, 55, 10–21. https://doi.org/10.1016/j.chiabu.2016.03.007
Blagg, H., Tulich, T., Hovane, V., Raye, D., Worrigal, T., & May, S. (2020). Understanding the role of Law and Culture in Aboriginal and/or Torres Strait Islander communities in responding to and preventing family violence, Ngarluma/Jaru/Gooniyandi (Hovane), Kimberley and Pilbara region, WA, Jabirr Jabirr/Bardi (Raye), Dampier Peninsula and Kimberley region, WA, Gooniyandi/Gija (Worrigal), Kimberley region, WA (Research report, 19/2020). ANROWS.
Boeckel, M. G., Wagner, A., & Grassi-Oliveira, R. (2017). The effects of intimate partner violence exposure on the maternal bond and PTSD symptoms of children. Journal of Interpersonal Violence, 32(7), 1127–1142. https://doi.org/10.1177/0886260515587667
Borges Jelinic, A. (2019). I loved him and he scared me: Migrant women, partner visas and domestic violence. Emotion, Space and Society, 32(May 2018), 100582. https://doi.org/10.1016/j.emospa.2019.100582
Bradley, A., & Dinan, T. (2010). A systematic review of hypothalamic-pituitary-adrenal axis function in schizophrenia: Implications for mortality. Journal of Psychopharmacology, 24(4), 91–118. https://doi.org/10.1177/1359786810385491
Bronfenbrenner, U. (1977). Towards an experimental ecology of human development. American Psychologist, 32(7), 513–531.
Bronfenbrenner, U. (1994). Ecological models of human development. In M. Gauvin & M. Cole (Eds.), Readings on the development of children (2nd ed.; pp. 37–43). Freeman.
Bronfenbrenner, U., & Morris, P. A. (2007). The bioecological model of human development. In R. M. Lerner & W. E. Damon (Eds.), Handbook of child psychology: Theoretical models of human development (pp. 793–828). Wiley.
Btoush, R., & Campbell, J. (2009). Ethical conduct in intimate partner violence research: Challenges and strategies. Nursing Outlook, 57(4), 210–216. https://doi:10.1016/j.outlook.2008.10.005
Buckley, H., Holt, S., & Whelan, S. (2007). Listen to me! Children’s experiences of domestic violence. Child Abuse Review, 16, 296–310. https://doi.org/10.1002/car.995
Calma, T., Dudgeon, P., & Bray, A. (2017). Aboriginal and Torres Strait Islander social and emotional wellbeing and mental health. Australian Psychologist, 52(4), 255–260. https://doi.org/10.1111/ap.12299
Campbell, K. A., Thomas, A. M., Cook, L. J., & Keenan, H. T. (2013). Resolution of intimate partner violence and child behavior problems after investigation for suspected child maltreatment. JAMA Pediatrics, 167(3), 236–242. https://doi.org/10.1001/2013.jamapediatrics.324
Campo, M. (2015). Children’s exposure to domestic and family violence: Key issues and responses. Australian Institute of Family Studies. https://aifs.gov.au/cfca/sites/default/files/publication-documents/cfca-36-children-exposure-fdv.pdf
Carline, A., & Easteal. P. (2014). Shades of grey: Domestic and sexual violence against women: Law reform and society. Routledge.
Carter, B., Paranjothy, S., Davies, A., & Kemp, A. (2020). Mediators and effect modifiers of the causal pathway between child exposure to domestic violence and internalizing behaviors among children and adolescents: A systematic literature review. Trauma, Violence, & Abuse. https://doi.org/10.1177/1524838020965964
Cassells, R., Cortis, N., Duncan, A., Eastman, C., Gao, G., Giuntoli, G., Katz, I., Keegan, M., Macvean, M., Mavisakalyan, A., Shlonsky, A., Skattebol, J., Smyth, C., & valentine, k. (2014). Keep them safe outcomes evaluation: Final report. Department of Premier and Cabinet. https://theirfuturesmatter.nsw.gov.au/__data/assets/pdf_file/0004/678946/KTS_Outcomes_Evaluation_Final_Report.pdf
Cattane, N., Rossi, R., Lanfredi, M., & Cattaneo, A. (2017). Borderline personality disorder and childhood trauma: Exploring the affected biological systems and mechanisms. BMC Psychiatry, 17(1), 221. https://doi.org/10.1186/s12888-017-1383-2
Chen, E., Turiano, N. A., Mroczek, D. K., & Miller, G. E. (2016). Association of reports of childhood abuse and all-cause mortality rates in women. JAMA Psychiatry, 73(9), 920–927. https://doi.org/10.1001/jamapsychiatry.2016.1786
Christensen, D., Davis, G., Draper, G., Mitrou, F., McKeown, S., Lawrence, D., McAullay, D., Pearson, G., Rikkers, W., & Zubrick, S. R. (2014). Evidence for the use of an algorithm in resolving inconsistent and missing Indigenous status in administrative data collections. Australian Journal of Social Issues, 49(4), 423–443. https://doi.org/10.1002/j.1839-4655.2014.tb00322.x
Cicchetti, D., & Valentino, K. (2006). An ecological transitional perspective on child maltreatment: Failure of the average expectable environment and its influence upon child development. In D. Cicchetti & D. J. Cohen, (Eds.), Developmental psychopathology (2nd ed.; pp. 129–201). Wiley.
Clark, A., Preen, D. B., Ng, J. Q., Semmens, J. B., & Holman, C. D. A. J. (2010). Is Western Australia representative of other Australian states and territories in terms of key socio-demographic and health economic indicators? Australian Health Review, 34(2), 210–215. https://doi.org/10.1071/AH09805
Clark, C., Smuk, M., Lain, D., Stansfeld, S. A., Carr, E., Head, J., & Vickerstaff, S. (2017). Impact of childhood and adulthood psychological health on labour force participation and exit in later life. Psychological Medicine, 47(9), 1597–1608. https://doi.org/10.1017/S0033291717000010
Cohen, S., Janicki-Deverts, D., & Miller, G. (2007). Psychological stress and disease. Journal of the American Medical Association, 298(14), 1685–1687. https://doi.org/10.1001/jama.298.14.1685
Colizzi, M., Lasalvia, A., & Ruggeri, M. (2020). Prevention and early intervention in youth mental health: Is it time for a multidisciplinary and trans-diagnostic model for care? International Journal of Mental Health Systems, 14(23). https://doi.org/10.1186/s13033-020-00356-9
Collins, J. (2013). Rethinking Australian immigration and immigrant settlement policy. Journal of Intercultural Studies, 34(2), 160–177. https://doi.org/10.1080/07256868.2013.781981
Collison, K. L., & Lynam, D. R. (2021). Personality disorders as predictors of intimate partner violence: A meta-analysis. Clinical Psychology Review, 88(August 2020), 102047. https://doi.org/10.1016/j.cpr.2021.102047
Colman, I., & Ataullahjan, A. (2010). Life course perspectives on the epidemiology of depression. Canadian Journal of Psychiatry, 55(10), 622–632. https://doi.org/10.1177/070674371005501002
Colman, I., Murray, J., Abbott, R. A., Maughan, B., Kuh, D., Croudace, T. J., & Jones, P. B. (2009). Outcomes of conduct problems in adolescence: 40-year follow-up of national cohort. BMJ (Online), 338(7688), 208–211. https://doi.org/10.1136/bmj.a2981
Commonwealth of Australia. (2015). Senate Standing Committees on Community Affairs: Out of home care report. https://www.aph.gov.au/Parliamentary_Business/Committees/Senate/Community_Affairs/Out_of_home_care/Report
Commonwealth of Australia. Department of the Prime Minister and Cabinet. (2021). National Agreement on Closing the Gap. Commonwealth of Australia.
Council of Australian Governments. (2011). National Plan to Reduce Violence against Women and their Children 2010–2022. https://www.dss.gov.au/women/programs-services/reducing-violence/the-national-plan-to-reduce-violence-against-women-and-their-children-2010-2022
Council of Australian Governments. (2015). National Outcome Standards for Perpetrator Interventions. https://plan4womenssafety.dss.gov.au/wp-content/uploads/2015/04/nospi_coag_paper.pdf
Council of Australian Governments. (2019). Fourth Action Plan of the National Plan to Reduce Violence against Women and their Children 2010–2022. https://www.dss.gov.au/women-publications-articles-reducing-violence/fourth-action-plan
Cox, P. (2015). Violence against women: Additional analysis of the Australian Bureau of Statistics’ Personal Safety Survey, 2012 (ANROWS Horizons, 01.01/2016, Rev. ed.). ANROWS.
Crosby, J. P., & Sprock, J. (2004). Effect of patient sex, clinician sex, and sex role on the diagnosis of antisocial personality disorder: Models of underpathologizing and overpathologizing biases. Journal of Clinical Psychology, 60(6), 583–604. https://doi.org/10.1002/jclp.10235
Crowley, R., Wolfe, I., Lock, K., & McKee, M. (2011). Improving the transition between paediatric and adult healthcare: A systematic review. Archives of Disease in Childhood, 96(6), 548–553. https://doi.org/10.1136/adc.2010.202473
Cunneen, C. (2010). Alternative and improved responses to domestic and family violence in Queensland Indigenous communities. University of New South Wales. https://documents.parliament.qld.gov.au/TableOffice/TabledPapers/2010/5310T1801.pdf
D’Andrea, W., & Graham-Berman, S. (2017). Social context and violence exposure as predictors of internalizing symptoms in mothers and children exposed to intimate partner violence. Journal of Family Violence, 32(2), 145–155. https://doi.org/10.1007/s10896-016-9869-0
Dababnah, S., Rizo, C. F., Campion, K., Downton, K. D., & Nichols, H. M. (2018). The relationship between children’s exposure to intimate partner violence and intellectual and developmental disabilities: A systematic review of the literature. American Journal on Intellectual and Developmental Disabilities, 123(6), 529–544. https://doi.org/10.1352/1944-7558-123.6.529
Dahlberg, L.L., & Krug, E.G. (2002). Violence – A global public health problem. In: E.G. Krug et al. (Eds.), World report on violence and health (pp. 3–21). World Health Organization.
Devaney, J. (2015). Research review: The impact of domestic violence on children. Irish Probation Journal, 12, 79–94.
Dobash, R. P., & Dobash, R. E. (1979). Violence against wives: A case against the patriarchy. Free Press.
Dudgeon, P., Calma, T., & Holland, C. (2017). The context and causes of the suicide of Indigenous people in Australia. Journal of Indigenous Wellbeing: Te Mauri, 2(2), 5–15. https://journalindigenouswellbeing.com/journal_articles/the-context-and-causes-of-the-suicide-of-indigenous-people-in-australia/
du Plessis, B., Kaminer, D., Hardy, A., & Benjamin, A. (2015). The contribution of different forms of violence exposure to internalizing and externalizing symptoms among young South African adolescents. Child Abuse & Neglect, 45, 80–89. https://doi.org/10.1016/j.chiabu.2015.02.021
Ehrensaft, M. K., Cohen, P., Brown, J., Smailes, E., Chen, H., & Johnson, J. G. (2003). Intergenerational transmission of partner violence: A 20-year prospective study. Journal of Consulting and Clinical Psychology, 71(4), 741–753. https://doi.org/10.1037/0022-006x.71.4.741
Ellsberg, M., & Heise, L. (2005) Researching violence against women: A practical guide for researchers and activists. World Health Organization.
Emerson, E., & Hatton, C. (2007). Mental health of children and adolescents with intellectual disabilities in Britain. British Journal of Psychiatry, 191(December), 493–499. https://doi.org/10.1192/bjp.bp.107.038729
Erskine, H. E., Norman, R. E., Ferrari, A. J., Chan, G. C. K., Copeland, W. E., Whiteford, H. A., & Scott, J. G. (2016). Long-term outcomes of attention-deficit/hyperactivity disorder and conduct disorder: A systematic review and meta-analysis. Journal of the American Academy of Child and Adolescent Psychiatry, 55(10), 841–850. https://doi.org/10.1016/j.jaac.2016.06.016
European Institute for Gender Inequality. (2017). Glossary of definitions of rape, femicide and intimate partner violence. https://eige.europa.eu/publications/glossary-definitions-rape-femicide-and-intimate-partner-violence
Evans, M. A., & Feder, G. S. (2016). Help-seeking amongst women survivors of domestic violence: A qualitative study of pathways towards formal and informal support. Health Expectations: An International Journal of Public Participation in Health Care and Health Policy, 19(1), 62–73. https://doi.org/10.1111/hex.12330
Evans, S. E., Davies, C., & Dilillo, D. (2008). Exposure to domestic violence: A meta-analysis of child and adolescent outcomes. Aggression and Violent Behavior, 13, 131–140.
Fantuzzo, J. W., & Lindquist, C. U. (1989). The effects of observing conjugal violence on children: A review and analysis of research methodology. Journal of Family Violence, 4(1), 77–94. https://doi.org/10.1007/BF00985658
Fergusson, D. M., Horwood, L. J., & Ridder, E. M. (2007). Conduct and attentional problems in childhood and adolescence and later substance use, abuse and dependence: Results of a 25-year longitudinal study. Drug and Alcohol Dependence, 88(Suppl.1), 14–26. https://doi.org/10.1016/j.drugalcdep.2006.12.011
Fisher, C. (2013). Changed and changing gender and family roles and domestic violence in African refugee background communities post-settlement in Perth, Australia. Violence Against Women, 19(7), 833–847. https://doi.org/10.1177/1077801213497535
Fisher, C., McKenzie, A., Preen, D., and Crowe, S., Cooke, V., Glauert, R., O’Donnell, M., Adams, I., West, M., Smith, S., Harrison, H., Nguyen, R., Henning, L., McNeil, N., & Frank, B. (2016). Family and domestic violence priority setting partnership project report. The University of Western Australia School of Population Health, Telethon Kids Institute, Kulunga Aboriginal Research Development Unit, Consumer and Community Health Research Network, Anglicare WA, Crowe Associates. https://www.anglicarewa.org.au/docs/default-source/who-we-are/research—family-and-communities/family-and-domestic-violence-priority-setting-partnership-project-report.pdf?sfvrsn=4d80ba5_2
Forns, M., Abad, J., & Kirchner T. (2018). Internalizing and externalizing problems. In R.J.R. Levesque (Ed.), Encyclopedia of adolescence. Springer. https://doi.org/10.1007/978-3-319-33228-4_261
Fraga, S. (2016). Methodological and ethical challenges in violence research. Porto Biomedical Journal, 1(2), 77–80. https://doi.org/10.1016/j.pbj.2016.04.005
Francis, L., Loxton, D., & James, C. (2017). The culture of pretence: A hidden barrier to recognising, disclosing and ending domestic violence. Journal of Clinical Nursing, 26(15–16), 2202–2214. https://doi.org/10.1111/jocn.13501
García-Moreno, C., Jansen, H.A., Ellsberg, M., Heise, L., & Watts, C. (2005). WHO multi-country study on women’s health and domestic violence against women: Initial results on prevalence, health outcomes and women’s responses. World Health Organization.
García-Moreno, C., Hegarty, K., d’Oliveira, A., Koziol-McLain, J., Colombini, M., & Feder, G. (2015). The health-systems response to violence against women. Lancet, 385(9977), 1567–1579. https://doi.org/10.1016/S0140-6736(14)61837-7
Gartland, D., Conway, L. J., Giallo, R., Mensah, F. K., Cook, F., Hegarty, K., Herrman, H., Nicholson, J., Reilly, S., Hiscock, H., Sciberras, E., & Brown, S. J. (2021). Intimate partner violence and child outcomes at age 10: A pregnancy cohort. Archives of Disease in Childhood, 1–9. https://doi.org/10.1136/archdischild-2020-320321
Gezinski, L. B., Gonzalez-Pons, K. M., & Rogers, M. M. (2021). Substance use as a coping mechanism for survivors of intimate partner violence: Implications for safety and service accessibility. Violence Against Women, 27(2), 108–123. https://doi.org/10.1177/1077801219882496
Ghafournia, N., & Easteal, P. (2018). Are immigrant women visible in Australian domestic violence reports that potentially influence policy? Laws, 7(4), 32. https://doi.org/10.3390/laws7040032
Gilbert, R., Widom, C. S., Browne, K., Fergusson, D., Webb, E., & Janson, S. (2009). Burden and consequences of child maltreatment in high-income countries. Lancet, 373(9657), 68–81.
Glasson, E. J., de Klerk, N. H., Bass, A. J. Rosman, D. L., Palmer, L. J., & Holman, C. D. J. (2008). Cohort profile: The Western Australian Family Connections Genealogical Project. International Journal of Epidemiology, 37(1), 30–35. https://doi.org/10.1093/ije/dym136
Goodsell, B., Lawrence, D., Ainley, J., Sawyer, M., Zubrick, S., & Maratos, J. (2017). Child and adolescent mental health and educational outcomes: An analysis of educational outcomes from Young Minds Matter: The second Australian Child and Adolescent Survey of Mental Health and Wellbeing. Young Minds Matter. https://youngmindsmatter.telethonkids.org.au/siteassets/media-docs—young-minds-matter/childandadolescent-mentalhealthandeducationaloutcomesdec2017.pdf
Government of Western Australia. (2015). Western Australian Family and Domestic Violence Common Risk Assessment and Risk Management Framework. https://www.wa.gov.au/government/document-collections/western-australian-family-and-domestic-violence-common-risk-assessment-and-risk-management-framework
Government of Western Australia. (2021b). Aboriginal Empowerment Strategy – Western Australia 2021–2029. https://www.wa.gov.au/organisation/department-of-the-premier-and-cabinet/aboriginal-empowerment-strategy-western-australia-2021-2029
Government of Western Australia Department of Health. (2022). Family connections. Data Linkage Western Australia. https://www.datalinkage-wa.org.au/dlb-services/family-connections/
Gracia, E., López-Quílez, A., Marco, M., & Lila, M. (2018). Neighborhood characteristics and violence behind closed doors: The spatial overlap of child maltreatment and intimate partner violence. PLOS One, 13(6), e0198684. https://doi.org/10.1371/journal.pone.0198684
Graham-Bermann, S. A. (2011). Child maltreatment in the context of intimate partner violence. In J. E. B. Myers (Ed.), The APSAC handbook on child maltreatment (3rd ed.; pp. 167–180). Sage.
Graham-Bermann, S. A., & Perkins, S. (2010). Effects of early exposure and lifetime exposure to intimate partner violence on child adjustment. Violence and Victims, 25(4), 427–439. https://doi.org/10.1891/0886-6708.25.4.427
Greene, C. A., Chan, G., McCarthy, K. J., Wakschlag, L. S., & Briggs-Gowan, M. J. (2018). Psychological and physical intimate partner violence and young children’s mental health: The role of maternal posttraumatic stress symptoms and parenting behaviors. Child Abuse & Neglect, 77, 168–179. https://doi.org/10.1016/j.chiabu.2018.01.012
Gray, R. J. (1988). A class of K-sample tests for comparing the cumulative incidence of a competing risk. Annals of Statistics,16, 1141–1154.
Hafekost, K., Lawrence, D., O’Leary, C., Bower, C., O’Donnell, M., Semmens, J., & Zubrick, S. R. (2017). Maternal alcohol use disorder and subsequent child protection contact: A record-linkage population cohort study. Child Abuse & Neglect, 72, 206–214. https://doi.org/10.1016/j.chiabu.2017.08.010
Hancock, K. J., Lawrence, D., Shepherd, C. C. J., Mitrou, F., & Zubrick, S. R. (2017). Associations between school absence and academic achievement: Do socioeconomics matter? British Educational Research Journal, 43(3), 415–440. https://doi.org/10.1002/berj.3267
Hansen, D., Lou, H.C., & Olsen, J. (2000). Serious life events and congenital malformations: A national study with complete follow-up. Lancet, 356(9233), 875–880.
Harron, K., Dibben, C., Boyd, J., Hjern, A., Azimaee, M., Barreto, M. L., & Goldstein, H. (2017). Challenges in administrative data linkage for research. Big Data & Society, 4(2). https://doi.org/10.1177/2053951717745678
Harvey, A., García-Moreno, C., & Butchart, A. (2007). Primary prevention of intimate partner violence and sexual violence: Background paper for WHO Expert Meeting May 2–3, 2007. World Health Organization. https://www.who.int/violence_injury_prevention/publications/violence/IPV-SV.pdf
Hebron, J., & Humphrey, N. (2014). Mental health difficulties among young people on the autistic spectrum in mainstream secondary schools: A comparative study. Journal of Research in Special Educational Needs, 14(1), 22–32. https://doi.org/10.1111/j.1471-3802.2012.01246.x
Heise, L. L. (1998). Violence against women: An integrated, ecological framework. Violence Against Women, 4(3), 262–290. https://doi.org/10.1177/1077801298004003002
Henderson, D. X., DeCuir-Gunby, J., & Gill, V. (2016). “It really takes a village”: A socio-ecological model of resilience for prevention among economically disadvantaged ethnic minority youth. Journal of Primary Prevention, 37, 469–485. https://doi.org/10.1007/s10935-016-0446-3
Herrman, H., Stewart, D. E., Diaz-Granados, N., Berger, E. L., Jackson, B., & Yuen, T. (2011). What is resilience? Canadian Journal of Psychiatry, 56(5), 258–265. https://doi.org/10.1177/070674371105600504
Herrenkohl, T. I., Sousa, C., Tajima, E. A., Herrenkohl, R. C., & Moylan, C. A. (2008). Intersection of child abuse and children’s exposure to domestic violence. Trauma, Violence & Abuse, 9, 84–99.
Hertzman, C., & Williams, R. (2009). Making early childhood count. Canadian Medical Association Journal, 180(1), 68–71. https://doi.org/10.1503/cmaj.080512
Heward-Belle, S., Humphreys, C., Healey, L., Toivonen, C., & Tsantefski, M. (2019). Invisible practices: Interventions with men who use violence and control. Affilia, 34(3), 369–382. https://doi.org/10.1177/0886109919848750
Hindmarsh, G., Laurens, K. R., Katz, I., Butler, M., Harris, F., Carr, V. J., & Green, M. J. (2021). Child protection services for children with special healthcare needs: A population record linkage study. Australian Journal of Social Issues, 56(2), 223–243. https://doi.org/10.1002/ajs4.145
Holden, G. W. (2003). Children exposed to domestic violence and child abuse: Terminology and taxonomy. Clinical Child and Family Psychology Review, 6, 151–160. https://doi.org/10.1023/A:1024906315255
Holman, C. D. J., Bass, A. J., Rosman, D. L., Smith, M. B., Semmens, J. B., Glasson, E. J., Brook, E. L., Trutwein, B., Rouse, I. L., Watson, C. R., de Klerk, N. H., Stanley, F. J., & Holman, C. J. (2008). A decade of data linkage in Western Australia: Strategic design, applications and benefits of the WA Data Linkage System. Australian Health Review, 32(4), 766–777. https://doi.org/10.1071/AH080766
Holman, C. D., Bass, A. J., Rouse, I. L., & Hobbs, M. S. (1999). Population-based linkage of health records in Western Australia: Development of a health services research linked database. Australian and New Zealand Journal of Public Health, 23(5), 453–459.
Holmes, M. R., Voith, L. A., & Gromoske, A. N. (2015). Lasting effect of intimate partner violence exposure during preschool on aggressive behavior and prosocial skills. Journal of Interpersonal Violence, 30(10), 1651–1670. https://doi.org/10.1177/0886260514552441
Hosokawa, R., & Katsura, T. (2019). Exposure to marital conflict: Gender differences in internalizing and externalizing problems among children. PLOS One, 14(9), 1–14. https://doi.org/10.1371/journal.pone.0222021
Howarth, E., Moore, T., Welton, N., Lewis, N., Stanley, N., MacMillan, H., Shaw, A., Hester, M., Bryden, P., & Feder, G. (2016). IMPRoving Outcomes for children exposed to domestic ViolencE (IMPROVE): An evidence synthesis. Public Health Research, 4(10), 1–342. https://doi.org/10.3310/phr04100
Howell, K. (2011). Resilience and psychopathology in children exposed to family violence. Aggression and Violent Behavior, 16(6), 562–569. https://doi.org/10.1016/j.avb.2011.09.001
Huang, C. C., Chen, Y., & Cheung, S. (2021). Early childhood exposure to intimate partner violence and teen depression symptoms in the U.S. Health and Social Care in the Community, 29(5), e47–e55. https://doi.org/10.1111/hsc.13240
Hultmann, O., & Broberg, A. G. (2016). Family violence and other potentially traumatic interpersonal events among 9- to 17-year-old children attending an outpatient psychiatric clinic. Journal of Interpersonal Violence, 31(18), 2958–2986. https://doi.org/10.1177/0886260515584335
Hultmann, O., Broberg, A. G., & Axberg, U. (2020). Child psychiatric patients exposed to intimate partner violence and/or abuse: The impact of double exposure. Journal of Interpersonal Violence 37(11–12), NP8611–NP8631. https://doi.org/10.1177/0886260520978186
Huth-Bocks, A. C., Levendosky, A. A., & Semel, M. A. (2001). The direct and indirect effects of domestic violence on young children’s intellectual functioning. Journal of Family Violence, 16, 269–290. https://doi.org/10.1023/A:1011138332712
Indermaur, D. (2001). Young Australians and domestic violence (Trends & Issues in Crime and Criminal Justice, no. 195). Australian Institute of Criminology. https://www.aic.gov.au/publications/tandi/tandi195
Izaguirre, A., & Calvete, E. (2018). Exposure to family violence and internalizing and externalizing problems among Spanish adolescents. Violence and Victims, 1(33), 368–382. https://doi.org/10.1891/0886-6708.VV-D-17-00016
Jackson, M. A., Sippel, L. M., Mota, N., Whalen, D., & Schumacher, J. A. (2015). Borderline personality disorder and related constructs as risk factors for intimate partner violence perpetration. Aggression and Violent Behavior, 24, 95–106. https://doi.org/10.1016/j.avb.2015.04.015
Jeffries, S., & Bond, C. E. (2015). Taking the problem seriously? Sentencing Indigenous and non-Indigenous domestic violence offenders. Australian & New Zealand Journal of Criminology, 48(4), 463–482. https://doi.org/10.1177/0004865814554306
Juruena, M. F., Eror, F., Cleare, A. J., & Young, A. H. (2020). The role of early life stress in HPA axis and anxiety. Advances in Experimental Medicine and Biology, 1191, 141–153. https://doi.org/10.1007/978-981-32-9705-0_9
Jutte, D. P., Roos, L., & Brownell, M.D. (2011). Administrative record linkage as a tool for public health research. Annual Review of Public Health, 32, 91–108.
Karakurt, G., Smith, D., & Whiting, J. (2014). Impact of intimate partner violence on women’s mental health. Journal of Family Violence, 29(7), 693–702.
Keeling, J., & Fisher, C. (2015). Health professionals’ responses to women’s disclosure of domestic violence. Journal of Interpersonal Violence, 30(13), 2363.
Kelman, C., Bass, A. J. & Holman, C. D. J. (2002). Research use of linked health data: A best practice protocol. Australian and New Zealand Journal of Public Health, 26(3), 251–255. https://doi.org/10.1111/j.1467-842X.2002.tb00682.x
Kennedy, A. C., Bybee, D., Sullivan, C. M., & Greeson, M. (2010). The impact of family and community violence on children’s depression trajectories: Examining the interactions of violence exposure, family social support, and gender. Journal of Family Psychology, 24(2), 197–207. https://doi.org/10.1037/a0018787
Kernic, M. A., Wolf, M. E., Holt, V. L., McKnight, B., Huebner, C. E., & Rivara, F. P. (2003). Behavioral problems among children whose mothers are abused by an intimate partner. Child Abuse & Neglect, 27(11), 1231–1246. https://doi.org/10.1016/j.chiabu.2002.12.001
Kessler, R. C., Berglund, P., Demler, O., Jin, R., Merikangas, K. R., & Walters, E. E. (2005). Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry, 62(6), 593–602. https://doi.org/10.1001/archpsyc.62.6.593
Kiecolt-Glaser, J., & Glaser, R. (2005). Stress-induced immune dysfunction: Implications for health. Nature Reviews Immunology, 5(3), 243–251. https://doi.org/10.1038/nri1571
Kimball, E. (2016). Edleson revisited: Reviewing children’s witnessing of domestic violence 15 years later. Journal of Family Violence, 31(5), 625–637. https://doi.org/10.1007/s10896-015-9786-7
Kitzmann, K. M., Gaylord, N. K., Holt, A. R., & Kenny, E. D. (2003). Child witnesses to domestic violence: A meta-analytic review. Journal of Consulting and Clinical Psychology, 71(2), 339–352. https://doi.org/10.1037/0022-006X.71.2.339
Kleinbaum, D. G., & Klein, M. (2012). Survival analysis: A self-learning text (3rd ed.). Springer.
Koenen, K., Moffitt, T., Caspi, A., Taylor, A., & Purcell, S. (2003). Domestic violence is associated with environmental suppression of IQ in young children. Development and Psychopathology, 15(2), 297–311. https://doi.org/10.1017/S0954579403000166
Korhonen, M., Luoma, I., Salmelin, R., & Tamminen, T. (2012). A longitudinal study of maternal prenatal, postnatal and concurrent depressive symptoms and adolescent well-being. Journal of Affective Disorders, 136, 680–692.
Leckning, B., Hirvonen, T., Armstrong, G., Carey, T. A., Westby, M., Ringbauer, A., & Robinson, G. (2020). Developing best practice guidelines for the psychosocial assessment of Aboriginal and Torres Strait Islander people presenting to hospital with self-harm and suicidal thoughts. Australian & New Zealand Journal of Psychiatry, 54(9), 874–882. https://doi.org/10.1177/0004867420924082
Leckning, B., Ringbauer, A., Robinson, G., Carey, T. A., Hirvonen, T., & Armstrong, G. (2019). Guidelines for best practice psychosocial assessment of Aboriginal and Torres Strait Islander people presenting to hospital with self-harm and suicidal thoughts. Menzies School of Health Research.
Lemerle, K., & Stewart, D. E. (2011). Resilience: Thriving beyond adversity. In S. Dillon & E. Mackinlay (Eds.), Meaningful music making for life series, book 3 (pp. 19–48). Cambridge Scholars Publishing.
Langdon, S., Armour, C., & Stringer, M. (2014). Adult experience of mental health outcomes as a result of intimate partner violence victimisation: A systematic review. European Journal of Psychotraumatology, 5(24794), 1–12. https://doi.org/10.3402/ejpt.v5.24794
Lawrence, D., Dawson, V., Houghton, S., Goodsell, B., & Sawyer, M. G. (2019). Impact of mental disorders on attendance at school. Australian Journal of Education, 63(1), 5–21. https://doi.org/10.1177/0004944118823576
Lawrence, D., Johnson, S., Hafekost, S., Boterhoven de Haan, K., Sawyer, M., Ainley, J., & Zubrick, S. (2015). The mental health of children and adolescents: Report on the Second Australian Child and Adolescent Survey of Mental Health and Wellbeing (Issue report). Department of Health.
Leis, J. A., Heron J, Stuart E. A., & Mendelson, T. (2014). Associations between maternal mental health and child emotional and behavioral problems: Does prenatal mental health matter? Journal of Abnormal Child Psychology, 42, 161–71.
Lipsky, S., Holt, V.L., Easterling, T.R., & Critchlow, C.W. (2003). Impact of police-reported intimate partner violence during pregnancy on birth outcomes. Obstetrics & Gynecology, 102(3), 557–564. https://doi.org/10.1016/S0029-7844(03)00573-8
Loxton, D., Townsend, N., Cavenagh, D., & Green, L. (2017). Measuring domestic violence in longitudinal research. Australian Government Department of Social Services. https://plan4womenssafety.dss.gov.au/wp-content/uploads/2018/07/Measuring-Domestic-Violence-in-Longitudinal-Research.pdf
Luthar, S. S., Cicchetti, D., & Becker, B. (2000). The construct of resilience: A critical evaluation and guidelines for future work. Child Development, 71(3), 543–562. https://doi.org/10.1111/1467-8624.00164
MacDonald, K., Fainman-Adelman, N., Anderson, K. K., & Iyer, S. N. (2018). Pathways to mental health services for young people: A systematic review. Social Psychiatry and Psychiatric Epidemiology, 53(10). https://doi.org/10.1007/s00127-018-1578-y
Maclean, M., Sims, S., Bower, C., Leonard, H., Stanley, F. J., & O’Donnell, M. (2017). Maltreatment risk among children with disabilities. Pediatrics, 139(4). https://doi.org/10.1542/peds.2016-1817
Maclean, M. J., Sims, S. A., & O’Donnell, M. (2019). Role of pre-existing adversity and child maltreatment on mental health outcomes for children involved in child protection: Population-based data linkage study. BMJ Open, 9(7), e029675. https://doi.org/10.1136/bmjopen-2019-029675
Maclean, M. J., Taylor, C. L., & O’Donnell, M. (2017). Relationship between out-of-home care placement history characteristics and educational achievement: A population level linked data study. Child Abuse & Neglect, 70(August 2017), 146–159. https://doi.org/10.1016/j.chiabu.2017.05.013
Maclean, M. J., Taylor, C. L., & O’Donnell, M. (2020). Adolescent education outcomes and maltreatment: The role of pre-existing adversity, level of child protection involvement, and school attendance. Child Abuse & Neglect, 109, 104721. https://doi.org/10.1016/j.chiabu.2020.104721
McGavock, L., & Spratt, T. (2017). Children exposed to domestic violence: Using adverse childhood experience scores to inform service response. British Journal of Social Work, 47(4), 1128–1146. https://doi.org/10.1093/bjsw/bcw073
McLeod, J. D., & Kaiser, K. (2004). Childhood emotional and behavioral problems and educational attainment. American Sociological Review, 9, 636–658.
McTavish, J. R., MacGregor, J. C. D., Wathen, C. N., & MacMillan, H. L. (2016). Children’s exposure to intimate partner violence: An overview. International Review of Psychiatry, 28(5), 504–518. https://doi.org/10.1080/09540261.2016.1205001
Marçal, K. E. (2021). Intimate partner violence exposure and adolescent mental health outcomes: The mediating role of housing insecurity. Journal of Interpersonal Violence, 1–21. https://doi.org/10.1177/08862605211043588
Margolin, G., & Gordis, E.B. (2000). The effects of family and community violence on children. Annual Review of Psychology, 51(1), 445–479.
Margolin, G., & Vickerman, K. (2007). Posttraumatic stress in children and adolescents exposed to family violence. Professional Psychology: Research and Practice, 38(6), 613–619. https://doi.org/10.1037/0735-7028.38.6.613
Marmot, M. (2011). Social determinants and the health of Indigenous Australians. Medical Journal of Australia, 194(10), 512–513.
Marshall, C., Semovski, V., & Stewart, S. L. (2020). Exposure to childhood interpersonal trauma and mental health service urgency. Child Abuse & Neglect, 106(March), 1–10. https://doi.org/10.1016/j.chiabu.2020.104464
Martinez-Torteya, C., Bogat, G. A., Levendosky, A. A., & Von Eye, A. (2015). The influence of prenatal intimate partner violence exposure on hypothalamic-pituitary-adrenal axis reactivity and childhood internalizing and externalizing symptoms. Development and Psychopathology, 28(1), 55–72. https://doi.org/10.1017/S0954579415000280
Mason, R., & O’Rinn, S. E. (2014). Co-occurring intimate partner violence, mental health, and substance use problems: A scoping review. Global Health Action, 7, 24815. https://doi.org/10.3402/gha.v7.24815
Masten, A. S. (2001) Ordinary magic: Resilience processes in development. American Psychologist, 56, 227–238.
Masten A. S. (2011). Resilience in children threatened by extreme adversity: Frameworks for research, practice, and translational synergy. Development and Psychopathology, 23(2), 493–506. https://doi.org/10.1017/S0954579411000198
Matijasevich, A., Murray, J., Cooper, P. J., Anselmi, L., Barros, A. J., Barros, F. C., & Santos, I. S. (2014). Trajectories of maternal depression and offspring psychopathology at 6 years: 2004 Pelotas cohort study. Journal of Affective Disorders, 174, 424–431. https://doi.org/10.1016/j.jad.2014.12.012
Mills, R., Scott, J., Alati, R., O’Callaghan, M., Najman, J. M., & Strathearn, L. (2012). Child maltreatment and adolescent mental health problems in a large birth cohort. Child Abuse & Neglect, 37(5), 292–302. https://doi.org/10.1016/j.chiabu.2012.11.008
Minas, H., Kakuma, R., Too, L. S., Vayani, H., Orapeleng, S., Prasad-Ildes, R., Turner, G., Procter, N., & Oehm, D. (2013). Mental health research and evaluation in multicultural Australia: Developing a culture of inclusion. Mental Health in Multicultural Australia (MHiMA), 7, Article 23. https://doi.org/10.1186/1752-4458-7-23
Moylan, C., Herrenkohl, T., Sousa, C., Tajima, E., Herrenkohl, R., & Russo, M. (2010). The effects of child abuse and exposure to domestic violence on adolescent internalizing and externalizing behavior problems. Journal of Family Violence, 25(1), 53–63. https://doi.org/10.1007/s10896-009-9269-9
Mueller, I., & Tronick, E. (2019). Early life exposure to violence: Developmental consequences on brain and behavior. Frontiers in Behavioral Neuroscience, 13, 156. https://doi.org/10.3389/fnbeh.2019.00156
Najman, J. M., Hayatbakhsh, M. R., Clavarino, A., Bor, W., O’Callaghan, M. J., & Williams, G. M. (2010). Family poverty over the early life course and recurrent adolescent and young adult anxiety and depression: A longitudinal study. American Journal of Public Health, 100(9), 1719–1723.
National Mental Health Commission. (2018). Australian Mental Health Commissions: Submission to the accessibility and quality of mental health services in rural and remote Australia Senate Inquiry [Submission]. https://www.nswmentalhealthcommission.com.au/sites/default/files/old/documents/mental_health_commissions_submission_-_mental_health_services_in_rural_and_remote_australia.pdf
National Mental Health Commission. (2020a). Children’s Mental Health and Wellbeing Strategy Consultations: January–February 2020. National Mental Health Commission.
National Mental Health Commission. (2020b). Inquiry into Family Domestic and Sexual Violence. https://www.mentalhealthcommission.gov.au/getmedia/f35003f4-5360-4f31-acee-efaa7c80c086/Submission-to-the-Inquiry-into-family-domestic-and-sexual-violence
National Scientific Council on the Developing Child. (2012). The science of neglect: The persistent absence of responsive care disrupts the developing brain. Center on the Developing Child: Harvard University.
Nock, M. K., Kazdin, A. E., Hiripi, E., & Kessler, R. C. (2007). Lifetime prevalence, correlates, and persistence of oppositional defiant disorder: Results from the National Comorbidity Survey Replication. Journal of Child Psychology and Psychiatry and Allied Disciplines, 48(7), 703–713. https://doi.org/10.1111/j.1469-7610.2007.01733.x
O’Donnell, M., Maclean, M. J., Sims, S., Morgan, V. A., Leonard, H., & Stanley, F. J. (2015). Maternal mental health and risk of child protection involvement: Mental health diagnoses associated with increased risk. Journal of Epidemiology and Community Health, 69(12), 1175–1183. https://doi.org/10.1136/jech-2014-205240
Olaya, B., Ezpeleta, L., de la Osa, N., Granero, R., & Doménech, J. M. (2010). Mental health needs of children exposed to intimate partner violence seeking help from mental health services. Children and Youth Services Review, 32(7), 1004–1011. https://doi.org/10.1016/j.childyouth.2010.03.028
Olofsson, N., Lindqvist, K., Gådin, K., Bråbäck, L., & Danielsson, I. (2011). Physical and psychological symptoms and learning difficulties in children of women exposed and non-exposed to violence: A population-based study. International Journal of Public Health, 56(1), 89–96. https://doi.org/10.1007/s00038-010-0165-0
Onyskiw, J. E. (2002). Health and use of health services of children exposed to violence in their families. Canadian Journal of Public Health, 93(6), 416–420. https://doi.org/10.1007/BF03405028
Ormhaug, S. M., Jensen, T. K., Hukkelberg, S. S., Holt, T., & Egeland, K. E. (2012). Children’s trauma, hidden or forgotten? An inquiry into the traumatic experiences of children and adolescents in child and adolescent mental health care. Tidsskrift for Norsk Psykologforening, 49, 234–240.
Orr, C., Fisher, C. M., Glauert, R., Preen, D. B., & O’Donnell, M. (2020). A demographic profile of mothers and their children who are victims of family and domestic violence: Using linked police and hospital admissions data. Journal of Interpersonal Violence, 37(1–2), NP500–NP525. https://doi.org/10.1177/0886260520916272
Orr, C., Fisher, C., Preen, D., Glauert, R., & O’Donnell, M. (2020). Exposure to family and domestic violence is associated with increased childhood hospitalisations. PLOS One, 15(8), e0237251. https://doi.org/10.1371/journal.pone.0237251
Orr, C., Fisher, C., Sims, S., Preen, D., Glauert, R., & O’Donnell, M. (2019). Hospitalisations for maternal assault are associated with increased risk of child protection involvement. Child Abuse & Neglect, 95. https://doi.org/10.1016/j.chiabu.2019.05.007
Orr, C., Kelty, E., Fisher, C., O’Donnell, M., Glauert, R., & Preen, D. (2022). The lasting impact of family and domestic violence on neonatal health outcomes. Manuscript submitted for publication.
Orr, C., O’Donnell, M., Fisher, C., Bell, M. Glauert, R., & Preen, D. (2021). School readiness of children exposed to family and domestic violence. Journal of Interpersonal Violence, 27(7), 713–732 https://doi.org/10.1177/08862605211050099
Orr, C., Preen., D., Fisher, C., Sims, S., & O’Donnell, M. (2019). Trends in hospital admissions for intimate partner violence in Australian mothers with children born from 1990 to 2009. Journal of Interpersonal Violence, 36(15–16), 6988–7017. https://doi.org/10.1177/0886260519832905
Ortega-García, J. A., Soldin, O. P., Sánchez-Sauco, M. F., Cánovas-Conesa, A., Gomaríz-Peñalver, V., Jaimes-Vega, D.C., Perales, J. E., Cárceles-Alvarez, A., Martínez-Ros, M. T., & Ruiz, D. (2013). Violence against women and gastroschisis: A case-control study. International Journal of Environmental Research and Public Health, 10(10), 5178–5190. https://doi.org/10.3390/ijerph10105178
Our Watch. (2018). Changing the picture: A national resource to support the prevention of violence against Aboriginal and Torres Strait Islander women and their children. https://apo.org.au/sites/default/files/resource-files/2018-07/apo-nid182621.pdf
Överlien, C., & Hydén, M. (2009). Children’s actions when experiencing domestic violence. Childhood, 16(4), 479–496. https://doi.org/10.1177/0907568209343757
Paavilainen, E., Lepistö, S., & Flinck, A. (2014). Ethical issues in family violence research in healthcare settings. Nursing Ethics, 21(1), 43–52. https://doi.org/10.1177/0969733013486794
Pearson, H. (2015). Massive study to follow 80,000 British babies cancelled. Nature, 526, 620–621.
Papendick, M., Bohner, G., & Windman, S. (2017). “Passive victim – strong survivor”? Perceived meaning of labels applied to women who were raped. PLOS One, 12(5), e0177550–e0177550. https://doi.org/10.1371/journal.pone.0177550
Pham, T. T. Le, Berecki-Gisolf, J., Clapperton, A., O’Brien, K. S., Liu, S., & Gibson, K. (2021). Definitions of culturally and linguistically diverse (CALD): A literature review of epidemiological research in Australia. International Journal of Environmental Research and Public Health, 18(2), 1–23. https://doi.org/10.3390/ijerph18020737
Phillips, J., & Vandenbroek, P. (2014). Domestic and family violence in Australia: An overview of the issues (Parliamentary Library Research Paper). Parliament of Australia. https://www.aph.gov.au/About_Parliament/Parliamentary_Departments/Parliamentary_Library/pubs/rp/rp1415/ViolenceAust
Porter, C., Palmier-Claus, J., Branitsky, A., Mensell, W., Harwick, H., & Varese, F. (2020). Childhood adversity and borderline personality disorder: A meta-analysis. Acta Psychiatrica Scandinavica, 141, 6–20.
Ravens-Sieberer, U., Otto, C., Kriston, L., Rothenberger, A., Döpfner, M., Herpertz-Dahlmann, B., Barkmann, C., Schön, G., Hölling, H., Schulte-Markwort, M., Klasen, F., & BELLA Study Group (2015). The longitudinal BELLA study: Design, methods and first results on the course of mental health problems. European Child & Adolescent Psychiatry, 24(6), 651–663. https://doi.org/10.1007/s00787-014-0638-4
Reef, J., Van Meurs, I., Verhulst, F.C., & Van Der Ende, J. (2010). Children’s problems predict adults’ DSM-IV disorders across 24 years. Journal of the American Academy of Child and Adolescent Psychiatry, 49(11), 1117–1124. https://doi.org/10.1016/j.jaac.2010.08.002
Reichel, D. (2017). Determinants of intimate partner violence in Europe: The role of socioeconomic status, inequality, and partner behavior. Journal of Interpersonal Violence, 32(12), 1853–1873. https://doi.org/10.1177/0886260517698951
Reif, K., & Jaffe, P. (2019). Remembering the forgotten victims: Child-related themes in domestic violence fatality reviews. Child Abuse & Neglect, 98(September). https://doi.org/10.1016/j.chiabu.2019.104223
Reupert, A. E., Maybery, D. J., & Kowalenko, N. M. (2012). Children whose parents have a mental illness: Prevalence, need and treatment. Medical Journal of Australia, 1(April), 7–9. https://doi.org/10.5694/mjao11.11200
Richard, L., Gauvin, L., & Raine, K. (2011). Ecological models revisited: Their uses and evolution in health promotion over two decades. Annual Review of Public Health, 32(1), 307–326. https://doi.org/10.1146/annurev-publhealth-031210-101141
Richards, K. (2011). Children’s exposure to domestic violence in Australia (Trends & Issues in Crime and Criminal Justice, no. 419). Australian Institute of Criminology. https://eprints.qut.edu.au/65037/1/kelly.pdf
Robinson, S., valentine, k., Newton, B. J., Smyth, C., & Parmenter, N. (2020). Violence prevention and early intervention for mothers and children with disability: Building promising practice (Research report, 16/2020). ANROWS.
Rogers, C. J., Forster, M., Grigsby, T. J., Albers, L., Morales, C., & Unger, J. B. (2021). The impact of childhood trauma on substance use trajectories from adolescence to adulthood: Findings from a longitudinal Hispanic cohort study. Child Abuse & Neglect, 120(July 2020), 105200. https://doi.org/10.1016/j.chiabu.2021.105200
Royal Australian and New Zealand College of Psychiatrists. (2016). Children of parents with mental illness. https://www.ranzcp.org/news-policy/policy-and-advocacy/position-statements/children-of-parents-with-mental-illness
Ruiz-Pérez, I., Plazaola-Castaño, J., & Vives-Cases, C. (2007). Methodological issues in the study of violence against women. Journal of Epidemiology and Community Health, 61(Suppl. 2), 26–31. https://doi.org/10.1136/jech.2007.059907
Schulte Holthausen, B., & Habel, U. (2018). Sex differences in personality disorders. Current Psychiatry Reports, 20(12), 107. https://doi.org/10.1007/s11920-018-0975-y
Secretariat of National Aboriginal and Islander Child Care. (2017). Strong families, safe kids: Family violence response and prevention for Aboriginal and Torres Strait Islander children and families. https://www.snaicc.org.au/wp-content/uploads/2017/09/Strong_Families_Safe_Kids-Sep_2017.pdf
Segal, L., Doidge, J., Armfield, J. M., Gnanamanickam, E. S., Preen, D. B., Brown, D. S., & Nguyen, H. (2021). Association of child maltreatment with risk of death during childhood in South Australia. JAMA Network Open, 4(6), e2113221. https://doi.org/10.1001/jamanetworkopen.2021.13221
Seng, J. S., Graham-Bermann, S. A., Clark, M. K., McCarthy, A. M., & Ronis D. L. (2005). Posttraumatic stress disorder and physical comorbidity among female children and adolescents: Results from service-use data. Pediatrics, 116, 767–776.
Shepherd, C.C.J., Li, J., Cooper, M.N., Hopkins, K.D., & Farrant, B.M. (2017). The impact of racial discrimination on the health of Australian Indigenous children aged 5–10 years: Analysis of national longitudinal data. International Journal for Equity in Health, 16(1), 1–12. https://doi.org/10.1186/s12939-017-0612-0
Sher, L., Siever, L. J., Goodman, M., McNamara, M., Hazlett, E. A., Koenigsberg, H. W., & New, A. S. (2015). Gender differences in the clinical characteristics and psychiatric comorbidity in patients with antisocial personality disorder. Psychiatry Research, 229(3), 685–689. https://doi.org/10.1016/j.psychres.2015.08.022
Singh, S. P. (2009). Transition of care from child to adult mental health services: The great divide. Current Opinion in Psychiatry, 22(4), 386–390. https://doi.org/10.1097/YCO.0b013e32832c9221
Smith, C. A., Ireland, T. O., Park, A., Elwyn, L., & Thornberry, T. P. (2011). Intergenerational continuities and discontinuities in intimate partner violence: A two-generational prospective study. Journal of Interpersonal Violence, 26(18), 3720–3752. https://doi.org/10.1177/0886260511403751
Smith, M. (2004). Parental mental health: Disruptions to parenting and outcomes for children. Child & Family Social Work, 9(1), 3–11. https://doi.org/10.1111/j.1365-2206.2004.00312.x
Spilsbury, J. C., Kahana, S., Drotar, D., Creeden, R., Flannery, D. J., & Friedman, S. (2008). Profiles of behavioral problems in children who witness domestic violence. Violence and Victims, 23(1), 3–17. https://doi.org/10.1891/0886-6708.23.1.3
Sternberg, K.J., Baradaran, L.P., Abbott, C.B., Lamb, M.E., & Guterman, E. (2006). Type of violence, age, and gender differences in the effects of family violence on children’s behavior problems: A mega-analysis. Developmental Review, 26(1), 89–112. https://doi.org/10.1016/j.dr.2005.12.001
Study of Environment on Aboriginal Resilience and Child Health Investigators. (2010). The Study of Environment on Aboriginal Resilience and Child Health (SEARCH): Study protocol. BMC Public Health, 10(1), 287–287. https://doi.org/10.1186/1471-2458-10-287
Swanston, J., Bowyer, L., & Vetere, A. (2014). Towards a richer understanding of school-age children’s experiences of domestic violence: The voices of children and their mothers. Clinical Child Psychology and Psychiatry, 19(2), 184–201. https://doi.org/10.1177/1359104513485082
Teager, W., Fox, S., & Stafford, N. (2019). How Australia can invest early and return more: A new look at the $15b cost and opportunity. Early Intervention Foundation, The Front Project & CoLab at the Telethon Kids Institute.
Udo, I. E., Sharps, P., Bronner, Y., & Hossain, M. B. (2016). Maternal intimate partner violence: Relationships with language and neurological development of infants and toddlers. Maternal and Child Health Journal, 20(7), 1424–1431. https://doi.org/10.1007/s10995-016-1940-1.
UNICEF. (2006). Behind closed doors: The impact of domestic violence on children. https://www.unicef.org/media/files/BehindClosedDoors.pdf
United Nations General Assembly. (1989). United Nations Convention on the Rights of the Child. https://humanrights. gov.au/our-work/childrens-rights/convention-rights-child
VicHealth. (2012). Disability and health inequalities in Australia. https://www.vichealth.vic.gov.au/media-and-resources/publications/disability-and-health-inequalities-in-australia
Vilariño, M., Amado, B. G., Vázquez, M. J., & Arce, R. (2018). Psychological harm in women victims of intimate partner violence: Epidemiology and quantification of injury in mental health markers. Psychosocial Intervention, 27(3), 145–152. https://doi.org/10.5093/pi2018a23
Vittinghoff, E., Glidden, D. V., Shiboski, S. C., & McCulloch, C. E. (2012). Regression methods in biostatistics: Linear, logistic, survival, and repeated measures models (2nd ed.). Springer.
von Elm, E., Altman, D. G., Egger, M., Pocock, S. J., Gøtzsche, P. C., & Vandenbroucke, J.P. (2008). STROBE Initiative: The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Journal of Clinical Epidemiology, 61(4), 344–349.
Vu, N. L., Jouriles, E. N., McDonald, R., & Rosenfield, D. (2016). Children’s exposure to intimate partner violence: A meta-analysis of longitudinal associations with child adjustment problems. Clinical Psychology Review, 46, 25–33. https://doi.org/10.1016/j.cpr.2016.04.003
Wadman, R., Botting, N., Durkin, K., & Conti-Ramsden, G. (2011). Changes in emotional health symptoms in adolescents with specific language impairment. International Journal of Language and Communication Disorders, 46(6), 641–656. https://doi.org/10.1111/j.1460-6984.2011.00033.x
Walter, M., Lovett, R., Maher, B., Williamson, B., Prehn, J., Bodkin-Andrews, G., & Lee, V. (2021). Indigenous data sovereignty in the era of big data and open data. Australian Journal of Social Issues, 56(2), 143–156. https://doi.org/10.1002/ajs4.141
Wilson, M., Jones, J., Butler, T., Simpson, P., Gilles, M., Baldry, E., Levy, M., & Sullivan, E. (2017). Violence in the lives of incarcerated Aboriginal mothers in Western Australia. Sage Open, 7(1). https://doi.org/10.1177/2158244016686814
World Health Organization. (2011a). World report on disability. https://www.who.int/disabilities/world_report/2011/report.pdf
World Health Organization. (2011b). ICD-10: International statistical classification of diseases and related health problems (10th rev.). WHO.
World Health Organization. (2014). Violence against women: Intimate partner and sexual violence against women (Fact sheet no. 239). WHO.
World Health Organization. (2018). Mental health: Strengthening our response. https://www.who.int/news-room/fact-sheets/detail/mental-health-strengthening-our-response
World Health Organization. (2020a). Violence against women and the girl child: Intimate partner violence. https://worlds-women-2020-data-undesa.hub.arcgis.com/apps/intimate-partner-violence/explore
World Health Organization. (2020b). The ecological framework. https://www.who.int/violenceprevention/approach/ecology/en/
World Health Organization. (2022). The VPA approach. https://www.who.int/groups/violence-prevention-alliance/approach
Ybarra, G. J., Wilkens, S. L., & Lieberman, A. F. (2007). The influence of domestic violence on preschooler behavior and functioning. Journal of Family Violence, 22(1), 33–42. https://doi.org/10.1007/s10896-006-9054-y
Yodanis, C. L. (2004). Gender inequality, violence against women, and fear: A cross-national test of the feminist theory of violence against women. Journal of Interpersonal Violence, 19, 655–675. https://doi.org/10.1177/0886260504263868
Zalsman, G., Oquendo, M. A., Greenhill, L., Goldberg, P. H., Kamali, M., Martin, A., & Mann, J. J. (2006). Neurobiology of depression in children and adolescents. Child and Adolescent Psychiatric Clinics of North America, 15(4), 843–868. https://doi.org/10.1016/j.chc.2006.05.010
Zubrick, S. R., Silburn, S. R., Lawrence, D. M., Mitrou, F. G., Dalby, R. B., Blair, E. M., Griffin, J., Milroy, H., De Maio, J. A., Cox, A., & Li, J. (2005). The Western Australian Aboriginal Child Health Survey (WAACHS). Curtin University of Technology, & Telethon Institute for Child Health Research. https://www.telethonkids.org.au/our-research/aboriginal-health/waachs/
Legislation
Children and Community Services Act 2004 (WA).
Family Law Act 1975 (Cth).
Restraining Orders Act 1997 (WA).
Appendix A:
Australian and New Zealand Standard Offence Classification codes used to categorise DFV
Description
Classification code
Murder
0111
Attempted murder
0121
Assault and injury
0211, 0212, 0213, 0299
Sexual assault
0311, 0312
Threatening behaviour
0532
Misuse of weapons
1122
Source: Australian Bureau of Statistics. (2011). Australian and New Zealand Standard Offence Classification (ANZSOC). https://www.abs.gov.au/ausstats/[email protected]/mf/1234.0
Appendix B:
The association of DFV exposure on the risk (adjusted hazard ratios) of childhood mental health diagnosis by subcategory
The tables below provide the adjusted hazard ratios and 95 per cent confidence intervals (CIs) for the risk associated with DFV exposure on specific mental health diagnosis groups (relating to Figure 2 in the report). Individual models were run for each group. Adjustments were made for Aboriginal and Torres Strait Islander status, sex, early gestation (<37 weeks), mother’s age at birth, father’s age at birth, maternal marital status at birth, SES, residential remoteness, disability and maternal mental health contact. Bolded text in tables denotes statistically significant estimates where the 95 per cent CIs did not include the null value.
Mental health contact with no diagnosis recorded
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
1.52 (1.42, 1.62)
No
Reference group
Other mental illness-related contacts
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
1.21 (0.94, 1.56)
No
Reference group
Intentional self-harm
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
1.59 (1.30, 1.96)
No
Reference group
Substance use disorder
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
1.99 (1.66, 2.38)
No
Reference group
Psychological development disorder
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
1.19 (1.06, 1.33)
No
Reference group
Depressive disorder
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
1.36 (1.11, 1.66)
No
Reference group
Anxiety disorder
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
1.49 (1.37, 1.63)
No
Reference group
Schizophrenia and psychoses
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
1.39 (1.19, 1.63)
No
Reference group
Personality disorder
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
1.76 (1.18, 2.61)
No
Reference group
Organic disorder
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
1.41 (0.97, 2.04)
No
Reference group
Appendix C:
The association of sociodemographic characteristics on the risk of childhood mental health diagnosis by subcategory in children exposed to DFV and not exposed to DFV
Anxiety disorder
Aboriginal and/or Torres Strait Islander
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Yes
0.98 (0.84, 1.14)
1.09 (0.96, 1.25)
No
Reference group
Reference group
Sex
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Female
1.36 (1.20, 1.55) c
1.48 (1.33, 1.65)
Male
Reference group
Reference group
Preterm
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
<37 weeks
0.94 (0.77, 1.14)
1.02 (0.85, 1.22)
>37 weeks
Reference group
Reference group
Mother’s age at birth
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
<20 years
0.77 (0.61, 0.98)
0.99 (0.80, 1.24)
20–29 years
0.77 (0.63, 0.93)
0.99 (0.85, 1.15)
30–39 years
Reference group
Reference group
40+ years
1.79 (0.93, 3.42)
1.42 (0.91, 2.21)
Father’s age at birth
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
<20 years
1.08 (0.79, 1.48)
1.25 (0.94, 1.67)
20–29 years
1.16 (0.96, 1.41)
1.11 (0.95, 1.29)
30–39 years
Reference group
Reference group
40+ years
0.99 (0.68, 1.45)
1.25 (0.98, 1.59)
Missing age
1.25 (1.00, 1.55)
1.21 (0.99, 1.48)
Maternal marital status at birth
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Never married
1.06 (0.91, 1.23)
1.30 (1.12, 1.50)
Divorced/separated
1.02 (0.66, 1.56)
1.63 (1.11, 2.39)
Unknown/not stated
1.22 (0.54, 2.73)
2.07 (1.10, 3.87)
Married/de facto/widowed
Reference group
Reference group
Socioeconomic status
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
1–Most disadvantaged
0.78 (0.56, 1.07)
1.14 (0.84, 1.55)
2
0.82 (0.59, 1.14)
1.06 (0.78, 1.46)
3
0.86 (0.61, 1.21)
1.02 (0.74, 1.42)
4
0.80 (0.55, 1.17)
0.92 (0.65, 1.32)
5–Least disadvantaged
Reference group
Reference group
Residential remoteness
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Major cities
1.19 (0.94, 1.50)
1.04 (0.87, 1.26)
Outer regional
0.81 (0.61, 1.08)
0.86 (0.69, 1.07)
Remote
0.91 (0.68, 1.22)
0.84 (0.66, 1.06)
Very remote
0.78 (0.59, 1.04)
0.79 (0.62, 1.00)
Inner regional
Reference group
Reference group
Maternal mental health contact b
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Yes
1.14 (1.00, 1.30)
1.59 (1.42, 1.79)
No
Reference group
Reference group
Child has disability
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Yes
1.31 (1.11, 1.54)
1.61 (1.39, 1.86)
No
Reference group
Reference group
Notes: a Adjusted for characteristics listed in table.
b Mother had a mental health diagnosis in HMDC or MHIS records that occurred prior to the child’s mental health contact.
c Bold text denotes statistically significant estimates where the 95 per cent CIs did not include the null value.
Psychological development disorder
Aboriginal and or Torres Strait Islander
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Yes
0.88 (0.72, 1.07)
1.04 (0.90, 1.22)
No
Reference group
Reference group
Sex
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Female
0.77 (0.65, 0.91) c
0.61 (0.54, 0.70)
Male
Reference group
Reference group
Preterm
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
<37 weeks
1.35 (1.08, 1.69)
1.02 (0.84, 1.25)
>37 weeks
Reference group
Reference group
Mother’s age at birth
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
<20 years
0.83 (0.60, 1.14)
1.21 (0.95, 1.55)
20–29 years
0.98 (0.75, 1.26)
0.93 (0.78, 1.10)
30–39 years
Reference group
Reference group
40+ years
1.43 (0.62, 3.30)
1.94 (1.29, 2.93)
Father’s age at birth
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
< 20 years
1.17 (0.77, 1.79)
0.93 (0.66, 1.31)
20–29 years
1.31 (1.01, 1.71)
1.06 (0.89, 1.26)
30–39 years
Reference group
Reference group
40+ years
1.45 (0.92, 2.28)
1.15 (0.88, 1.50)
Missing age
1.45 (1.08, 1.94)
1.17 (0.93, 1.47)
Maternal marital status at birth
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Never married
1.04 (0.86, 1.27)
1.18 (0.99, 1.40)
Divorced/separated
0.76 (0.40, 1.42)
1.89 (1.27, 2.82)
Unknown/not stated
1.69 (0.75, 3.80)
2.06 (1.06, 4.00)
Married/de facto/widowed
Reference group
Reference group
Socioeconomic status
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
1–Most disadvantaged
0.87 (0.57, 1.33)
1.64 (1.10, 2.46)
2
0.87 (0.56, 1.34)
1.57 (1.04, 2.36)
3
0.83 (0.53, 1.31)
1.34 (0.87, 2.04)
4
0.82 (0.50, 1.36)
1.33 (0.85, 2.08)
5–Least disadvantaged
Reference group
Reference group
Residential remoteness
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Major cities
1.48 (1.06, 2.05)
1.28 (1.02, 1.60)
Outer regional
1.15 (0.78, 1.69)
0.99 (0.76, 1.29)
Remote
1.20 (0.80, 1.80)
0.92 (0.69, 1.22)
Very remote
0.75 (0.50, 1.12)
0.95 (0.71, 1.27)
Inner regional
Reference group
Reference group
Maternal mental health contact b
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Yes
0.99 (0.84, 1.17)
1.36 (1.18, 1.56)
No
Reference group
Reference group
Child has disability
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Yes
2.67 (2.23, 3.20)
3.28 (2.86, 3.76)
No
Reference group
Reference group
Notes: a Adjusted for characteristics listed in table.
b Mother had a mental health diagnosis in HMDC or MHIS records that occurred prior to the child’s mental health contact.
c Bold text denotes statistically significant estimates where the 95 per cent CIs did not include the null value.
Depressive disorder
Aboriginal and/or Torres Strait Islander
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Yes
0.78 (0.55, 1.12)
1.02 (0.77, 1.35)
No
Reference group
Reference group
Sex
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Female
2.83 (2.04, 3.94) c
2.81 (2.16, 3.66)
Male
Reference group
Reference group
Preterm
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
<37 weeks
1.13 (0.73, 1.74)
0.74 (0.46, 1.18)
>37 weeks
Reference group
Reference group
Mother’s age at birth
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
<20 years
1.19 (0.66, 2.13)
1.06 (0.65, 1.71)
20–29 years
1.11 (0.68, 1.82)
1.02 (0.73, 1.41)
30–39 years
Reference group
Reference group
40+ years
1.18 (0.16, 8.87)
1.75 (0.68, 4.47)
Father’s age at birth
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
<20 years
0.88 (0.43, 1.80)
1.08 (0.54, 2.14)
20–29 years
0.99 (0.63, 1.56)
1.29 (0.93, 1.79)
30–39 years
Reference group
Reference group
40+ years
1.80 (0.84, 3.85)
1.41 (0.83, 2.37)
Missing age
1.06 (0.63, 1.78)
1.31 (0.83, 2.06)
Maternal marital status at birth
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Never married
1.10 (0.78, 1.55)
1.06 (0.76, 1.48)
Divorced/separated
0.28 (0.04, 2.01)
1.76 (0.77, 4.03)
Unknown/not stated
Count too small
2.16 (0.53, 8.81)
Married/de facto/widowed
Reference group
Reference group
Socioeconomic status
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
1–Most disadvantaged
1.05 (0.48, 2.32)
1.72 (0.75, 3.96)
2
1.09 (0.48, 2.44)
1.86 (0.80, 4.31)
3
0.83 (0.35, 1.98)
1.61 (0.67, 3.84)
4
0.62 (0.22, 1.71)
1.82 (0.74, 4.45)
5–Least disadvantaged
Reference group
Reference group
Residential remoteness
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Major cities
1.06 (0.63, 1.80)
1.03 (0.68, 1.56)
Outer regional
0.89 (0.47, 1.67)
1.36 (0.87, 2.13)
Remote
0.92 (0.47, 1.80)
0.91 (0.54, 1.53)
Very remote
0.79 (0.42, 1.50)
0.62 (0.35, 1.09)
Inner regional
Reference group
Reference group
Maternal mental health contact b
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Yes
1.14 (0.84, 1.54)
1.42 (1.09, 1.84)
No
Reference group
Reference group
Child has disability
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Yes
1.72 (1.20, 2.46)
1.11 (0.77, 1.60)
No
Reference group
Reference group
Notes: a Adjusted for characteristics listed in table.
b Mother had a mental health diagnosis in HMDC or MHIS records that occurred prior to the child’s mental health contact.
c Bold text denotes statistically significant estimates where the 95 per cent CIs did not include the null value.
Mental health contact with no diagnosis recorded
Aboriginal and/or Torres Strait Islander
Characteristic
DFV exposure adjusted hazard ratiosa (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Yes
1.08 (0.96, 1.22)
1.27 (1.15, 1.40) c
No
Reference group
Reference group
Sex
Characteristic
DFV exposure adjusted hazard ratiosa (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Female
0.84 (0.77, 0.92)
0.83 (0.77, 0.90)
Male
Reference group
Reference group
Preterm
Characteristic
DFV exposure adjusted hazard ratiosa (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
<37 weeks
1.19 (1.04, 1.36)
1.16 (1.02, 1.31)
>37 weeks
Reference group
Reference group
Mother’s age at birth
Characteristic
DFV exposure adjusted hazard ratiosa (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
<20 years
0.83 (0.69, 0.98)
1.26 (1.08, 1.47)
20–29 years
0.79 (0.69, 0.92)
1.05 (0.94, 1.17)
30–39 years
Reference group
Reference group
40+ years
1.17 (0.65, 2.09)
1.09 (0.76, 1.55)
Father’s age at birth
Characteristic
DFV exposure adjusted hazard ratiosa (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
<20 years
1.08 (0.87, 1.36)
1.05 (0.86, 1.29)
20–29 years
1.07 (0.92, 1.24)
1.01 (0.91, 1.13)
30–39 years
Reference group
Reference group
40+ years
1.19 (0.91, 1.54)
1.32 (1.11, 1.56)
Missing age
1.05 (0.89, 1.24)
1.17 (1.01, 1.34)
Maternal marital status at birth
Characteristic
DFV exposure adjusted hazard ratiosa (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Never married
1.02 (0.91, 1.14)
1.14 (1.02, 1.26)
Divorced/separated
1.36 (1.01, 1.83)
1.51 (1.12, 2.03)
Unknown/not stated
1.89 (1.20, 2.98)
1.85 (1.17, 2.91)
Married/de facto/widowed
Reference group
Reference group
Socioeconomic status
Characteristic
DFV exposure adjusted hazard ratiosa (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
1–Most disadvantaged
1.04 (0.79, 1.38)
1.77 (1.34, 2.35)
2
1.01 (0.75, 1.35)
1.77 (1.33, 2.36)
3
1.27 (0.95, 1.70)
1.74 (1.30, 2.34)
4
1.10 (0.80, 1.52)
1.73 (1.27, 2.35)
5–Least disadvantaged
Reference group
Reference group
Residential remoteness
Characteristic
DFV exposure adjusted hazard ratiosa (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Major cities
0.92 (0.77, 1.10)
0.93 (0.81, 1.07)
Outer regional
1.07 (0.88, 1.32)
1.02 (0.87, 1.19)
Remote
1.21 (0.98, 1.49)
1.23 (1.05, 1.44)
Very remote
0.99 (0.81, 1.21)
0.94 (0.79, 1.11)
Inner regional
Reference group
Reference group
Maternal mental health contact b
Characteristic
DFV exposure adjusted hazard ratiosa (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Yes
0.91 (0.82, 1.00)
1.23 (1.13, 1.35)
No
Reference group
Reference group
Child has disability
Characteristic
DFV exposure adjusted hazard ratiosa (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Yes
1.02 (0.89, 1.16)
1.52 (1.37, 1.69)
No
Reference group
Reference group
Notes: a Adjusted for characteristics listed in table.
b Mother had a mental health diagnosis in HMDC or MHIS records that occurred prior to the child’s mental health contact.
c Bold text denotes statistically significant estimates where the 95 per cent CIs did not include the null value.
Other mental illness-related contacts
Aboriginal and/or Torres Strait Islander
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Yes
0.72 (0.45, 1.17)
0.58 (0.32, 1.08)
No
Reference group
Reference group
Sex
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Female
2.00 (1.33, 3.00) c
3.91 (2.11, 7.25)
Male
Reference group
Reference group
Preterm
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
<37 weeks
1.14 (0.66, 1.97)
1.31 (0.59, 2.92)
>37 weeks
Reference group
Reference group
Mother’s age at birth
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
<20 years
0.98 (0.47, 2.04)
0.18 (0.05, 0.65)
20–29 years
0.97 (0.53, 1.76)
0.83 (0.43, 1.61)
30–39 years
Reference group
Reference group
40+ years
1.56 (0.20, 12.03)
Count too small
Father’s age at birth
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
<20 years
0.30 (0.06, 1.38)
2.82 (0.66, 11.93)
20–29 years
1.21 (0.66, 2.20)
1.30 (0.65, 2.61)
30–39 years
Reference group
Reference group
40+ years
1.99 (0.76, 5.17)
Count too small
Missing age
1.55 (0.79, 3.04)
2.28 (0.96, 5.45)
Maternal marital status at birth
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Never married
0.80 (0.50, 1.30)
2.26 (1.18, 4.31)
Divorced/separated
Count too small
Count too small
Unknown/not stated
3.61 (0.87, 14.94)
Count too small
Married/de facto/widowed
Reference group
Reference group
Socioeconomic status
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
1–Most disadvantaged
1.44 (0.44, 4.75)
0.93 (0.27, 3.19)
2
1.36 (0.40, 4.62)
0.94 (0.27, 3.30)
3
0.96 (0.26, 3.53)
0.64 (0.16, 2.59)
4
1.87 (0.51, 6.82)
0.70 (0.16, 3.13)
5–Least disadvantaged
Reference group
Reference group
Residential remoteness
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Major cities
1.34 (0.60, 3.00)
1.90 (0.67, 5.39)
Outer regional
1.85 (0.77, 4.42)
1.55 (0.48, 4.97)
Remote
1.47 (0.57, 3.80)
1.33 (0.37, 4.81)
Very remote
1.04 (0.41, 2.63)
0.63 (0.14, 2.95)
Inner regional
Reference group
Reference group
Maternal mental health contact b
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Yes
1.03 (0.69, 1.53)
2.23 (1.30, 3.82)
No
Reference group
Reference group
Child has disability
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Yes
2.49 (1.62, 3.84)
0.85 (0.36, 1.98)
No
Reference group
Reference group
Notes: a Adjusted for characteristics listed in table.
b Mother had a mental health diagnosis in HMDC or MHIS records that occurred prior to the child’s mental health contact.
c Bold text denotes statistically significant estimates where the 95 per cent CIs did not include the null value.
Intentional self-harm
Aboriginal and/or Torres Strait Islander
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Yes
1.36 (0.95, 1.96)
1.17 (0.86, 1.60)
No
Reference group
Reference group
Sex
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Female
2.81 (2.05, 3.87) c
3.20 (2.39, 4.28)
Male
Reference group
Reference group
Preterm
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
<37 weeks
0.84 (0.54, 1.32)
0.81 (0.51, 1.30)
>37 weeks
Reference group
Reference group
Mother’s age at birth
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
<20 years
0.56 (0.33, 0.95)
0.78 (0.48, 1.27)
20–29 years
0.68 (0.44, 1.06)
0.77 (0.54, 1.08)
30–39 years
Reference group
Reference group
40+ years
1.22 (0.16, 9.05)
2.10 (0.74, 5.93)
Father’s age at birth
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
<20 years
1.78 (0.87, 3.62)
1.09 (0.52, 2.29)
20–29 years
1.57 (0.95, 2.58)
1.34 (0.94, 1.91)
30–39 years
Reference group
Reference group
40+ years
1.43 (0.58, 3.56)
0.61 (0.29, 1.29)
Missing age
1.89 (1.12, 3.22)
1.71 (1.09, 2.69)
Maternal marital status at birth
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Never married
1.29 (0.93, 1.78)
1.10 (0.78, 1.56)
Divorced/separated
0.77 (0.24, 2.45)
0.91 (0.29, 2.90)
Unknown/not stated
Count too small
1.09 (0.15, 7.84)
Married/de facto/widowed
Reference group
Reference group
Socioeconomic status
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
1–Most disadvantaged
1.53 (0.55, 4.22)
1.03 (0.49, 2.16)
2
1.62 (0.58, 4.58)
1.08 (0.51, 2.28)
3
2.00 (0.70, 5.71)
0.86 (0.39, 1.92)
4
1.18 (0.36, 3.85)
0.98 (0.43, 2.27)
5–Least disadvantaged
Reference group
Reference group
Residential remoteness
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Major cities
0.85 (0.52, 1.40)
0.76 (0.50, 1.16)
Outer regional
0.48 (0.25, 0.93)
0.96 (0.60, 1.53)
Remote
0.79 (0.43, 1.44)
0.67 (0.39, 1.14)
Very remote
0.62 (0.35, 1.11)
0.78 (0.47, 1.30)
Inner regional
Reference group
Reference group
Maternal mental health contact b
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Yes
1.07 (0.80, 1.44)
1.42 (1.07, 1.87)
No
Reference group
Reference group
Child has disability
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Yes
1.55 (1.09, 2.21)
1.03 (0.69, 1.54)
No
Reference group
Reference group
Notes: a Adjusted for characteristics listed in table.
b Mother had a mental health diagnosis in HMDC or MHIS records that occurred prior to the child’s mental health contact.
c Bold text denotes statistically significant estimates where the 95 per cent CIs did not include the null value.
Substance use disorder
Aboriginal and/or Torres Strait Islander
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Yes
2.92 (2.05, 4.16) c
4.59 (3.13, 6.75)
No
Reference group
Reference group
Sex
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Female
1.10 (0.86, 1.40)
0.83 (0.64, 1.06)
Male
Reference group
Reference group
Preterm
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
<37 weeks
1.14 (0.82, 1.59)
1.21 (0.84, 1.74)
>37 weeks
Reference group
Reference group
Mother’s age at birth
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
<20 years
1.29 (0.81, 2.05)
0.95 (0.60, 1.50)
20–29 years
1.04 (0.69, 1.57)
0.89 (0.62, 1.27)
30–39 years
Reference group
Reference group
40+ years
1.00 (0.14, 7.38)
0.97 (0.23, 4.10)
Father’s age at birth
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
<20 years
0.89 (0.51, 1.57)
0.87 (0.44, 1.70)
20–29 years
0.76 (0.51, 1.15)
1.11 (0.76, 1.61)
30–39 years
Reference group
Reference group
40+ years
1.29 (0.62, 2.70)
1.10 (0.55, 2.20)
Missing age
1.37 (0.91, 2.08)
1.79 (1.18, 2.71)
Maternal marital status at birth
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Never married
0.99 (0.75, 1.30)
1.22 (0.90, 1.65)
Divorced/separated
0.75 (0.27, 2.03)
0.78 (0.25, 2.47)
Unknown/not stated
0.83 (0.12, 5.94)
3.63 (1.33, 9.89)
Married/de facto/widowed
Reference group
Reference group
Socioeconomic status
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
1–Most disadvantaged
1.08 (0.52, 2.23)
0.80 (0.40, 1.59)
2
0.78 (0.36, 1.67)
0.43 (0.20, 0.91)
3
0.83 (0.38, 1.84)
0.52 (0.24, 1.14)
4
1.11 (0.47, 2.60)
0.91 (0.41, 2.00)
5–Least disadvantaged
Reference group
Reference group
Residential remoteness
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Major cities
1.17 (0.73, 1.87)
0.94 (0.60, 1.45)
Outer regional
0.78 (0.45, 1.35)
0.73 (0.44, 1.20)
Remote
0.78 (0.45, 1.36)
0.58 (0.34, 0.99)
Very remote
0.59 (0.35, 0.99)
0.64 (0.39, 1.06)
Inner regional
Reference group
Reference group
Maternal mental health contact b
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Yes
0.86 (0.67, 1.10)
1.28 (0.98, 1.67)
No
Reference group
Reference group
Child has disability
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Yes
1.80 (1.37, 2.38)
1.75 (1.28, 2.38)
No
Reference group
Reference group
Notes: a Adjusted for characteristics listed in table.
b Mother had a mental health diagnosis in HMDC or MHIS records that occurred prior to the child’s mental health contact.
c Bold text denotes statistically significant estimates where the 95 per cent CIs did not include the null value.
Schizophrenia and psychoses
Aboriginal and/or Torres Strait Islander
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Yes
0.98 (0.74, 1.29)
1.26 (1.00, 1.57)
No
Reference group
Reference group
Sex
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Female
1.95 (1.54, 2.48) c
2.08 (1.72, 2.53)
Male
Reference group
Reference group
Preterm
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
<37 weeks
0.98 (0.69, 1.39)
0.59 (0.40, 0.87)
>37 weeks
Reference group
Reference group
Mother’s age at birth
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
<20 years
1.51 (0.94, 2.41)
0.94 (0.65, 1.36)
20–29 years
1.34 (0.89, 2.02)
0.95 (0.73, 1.22)
30–39 years
Reference group
Reference group
40+ years
1.88 (0.44, 7.94)
1.51 (0.69, 3.30)
Father’s age at birth
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
<20 years
0.98 (0.57, 1.67)
1.08 (0.64, 1.81)
20–29 years
0.98 (0.69, 1.41)
1.12 (0.87, 1.45)
30–39 years
Reference group
Reference group
40+ years
1.64 (0.86, 3.14)
1.23 (0.80, 1.87)
Missing age
1.22 (0.81, 1.82)
1.41 (1.01, 1.98)
Maternal marital status at birth
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Never married
1.06 (0.82, 1.38)
1.08 (0.83, 1.39)
Divorced/separated
0.53 (0.17, 1.67)
1.50 (0.77, 2.95)
Unknown/not stated
1.63 (0.40, 6.60)
2.58 (0.95, 6.98)
Married/de facto/widowed
Reference group
Reference group
Socioeconomic status
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
1–Most disadvantaged
1.06 (0.57, 1.99)
1.41 (0.78, 2.56)
2
0.96 (0.50, 1.84)
1.47 (0.80, 2.68)
3
0.85 (0.43, 1.68)
1.19 (0.63, 2.24)
4
0.63 (0.28, 1.41)
1.41 (0.73, 2.71)
5–Least disadvantaged
Reference group
Reference group
Residential remoteness
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Major cities
1.06 (0.71, 1.60)
1.12 (0.80, 1.57)
Outer regional
0.84 (0.51, 1.37)
1.32 (0.91, 1.90)
Remote
0.89 (0.54, 1.48)
0.89 (0.59, 1.34)
Very remote
0.70 (0.43, 1.13)
0.75 (0.49, 1.15)
Inner regional
Reference group
Reference group
Maternal mental health contact b
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Yes
0.92 (0.73, 1.17)
1.44 (1.17, 1.76)
No
Reference group
Reference group
Child has disability
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Yes
1.53 (1.16, 2.03)
1.27 (0.97, 1.66)
No
Reference group
Reference group
Notes: a Adjusted for characteristics listed in table.
b Mother had a mental health diagnosis in HMDC or MHIS records that occurred prior to the child’s mental health contact.
c Bold text denotes statistically significant estimates where the 95 per cent CIs did not include the null value.
Personality disorder
Aboriginal and/or Torres Strait Islander
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Yes
0.72 (0.45, 1.17)
1.09 (0.96, 1.25)
No
Reference group
Reference group
Sex
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Female
2.00 (1.33, 3.00) c
1.48 (1.33, 1.65)
Male
Reference group
Reference group
Preterm
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
<37 weeks
1.14 (0.66, 1.97)
1.02 (0.85, 1.22)
>37 weeks
Reference group
Reference group
Mother’s age at birth
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
<20 years
0.98 (0.47, 2.04)
0.99 (0.80, 1.24)
20–29 years
0.97 (0.53, 1.76)
0.99 (0.85, 1.15)
30–39 years
Reference group
Reference group
40+ years
1.56 (0.20, 12.03)
1.42 (0.91, 2.21)
Father’s age at birth
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
<20 years
0.30 (0.06, 1.38)
1.25 (0.94, 1.67)
20–29 years
1.21 (0.66, 2.20)
1.11 (0.95, 1.29)
30–39 years
Reference group
Reference group
40+ years
1.99 (0.76, 5.17)
1.25 (0.98, 1.59)
Missing age
1.55 (0.79, 3.04)
1.21 (0.99, 1.48)
Maternal marital status at birth
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Never married
0.80 (0.50, 1.30)
1.30 (1.12, 1.50)
Divorced/separated
Count too small
1.63 (1.11, 2.39)
Unknown/not stated
3.61 (0.87, 14.94)
2.07 (1.10, 3.87)
Married/de facto/widowed
Reference group
Reference group
Socioeconomic status
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
1–Most disadvantaged
1.44 (0.44, 4.75)
1.14 (0.84, 1.55)
2
1.36 (0.40, 4.62)
1.06 (0.78, 1.46)
3
0.96 (0.26, 3.53)
1.02 (0.74, 1.42)
4
1.87 (0.51, 6.82)
0.92 (0.65, 1.32)
5–Least disadvantaged
Reference group
Reference group
Residential remoteness
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Major cities
1.34 (0.60, 3.00)
1.04 (0.87, 1.26)
Outer regional
1.85 (0.77, 4.42)
0.86 (0.69, 1.07)
Remote
1.47 (0.57, 3.80)
0.84 (0.66, 1.06)
Very remote
1.04 (0.41, 2.63)
0.79 (0.62, 1.00)
Inner regional
Reference group
Reference group
Maternal mental health contact b
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Yes
1.03 (0.69, 1.53)
1.59 (1.42, 1.79)
No
Reference group
Reference group
Child has disability
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Yes
2.49 (1.62, 3.84)
1.61 (1.39, 1.86)
No
Reference group
Reference group
Notes: a Adjusted for characteristics listed in table.
b Mother had a mental health diagnosis in HMDC or MHIS records that occurred prior to the child’s mental health contact.
c Bold text denotes statistically significant estimates where the 95 per cent CIs did not include the null value.
Organic disorder
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Aboriginal and/or Torres Strait Islander
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Yes
1.36 (0.71, 2.60)
0.88 (0.53, 1.47)
No
Reference group
Reference group
Sex
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Female
0.59 (0.33, 1.05)
0.50 (0.32, 0.79)
Male
Reference group
Reference group
Preterm
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
<37 weeks
0.93 (0.41, 2.09)
0.72 (0.31, 1.66)
>37 weeks
Reference group
Reference group
Mother’s age at birth
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
<20 years
0.42 (0.16, 1.13)
2.30 (0.91, 5.82)
20–29 years
0.58 (0.28, 1.21)
1.93 (1.04, 3.59) c
30–39 years
Reference group
Reference group
40+ years
Count too small
3.65 (0.78, 17.03)
Father’s age at birth
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
<20 years
0.94 (0.22, 3.98)
0.87 (0.28, 2.74)
20–29 years
1.01 (0.45, 2.29)
0.89 (0.52, 1.51)
30–39 years
Reference group
Reference group
40+ years
0.96 (0.21, 4.37)
0.50 (0.14, 1.78)
Missing age
1.55 (0.65, 3.71)
0.60 (0.23, 1.52)
Maternal marital status at birth
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Never married
1.06 (0.56, 2.02)
0.81 (0.42, 1.57)
Divorced/separated
1.28 (0.30, 5.47)
1.98 (0.48, 8.27)
Unknown/not stated
Count too small
Count too small
Married/de facto/widowed
Reference group
Reference group
Socioeconomic status
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
1–Most disadvantaged
0.76 (0.22, 2.61)
1.54 (0.36, 6.56)
2
0.52 (0.14, 1.97)
2.01 (0.47, 8.58)
3
0.68 (0.18, 2.67)
1.44 (0.32, 6.56)
4
0.88 (0.21, 3.70)
2.17 (0.47, 9.95)
5–Least disadvantaged
Reference group
Reference group
Residential remoteness
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Major cities
1.70 (0.60, 4.84)
1.41 (0.67, 2.99)
Outer regional
0.44 (0.10, 1.97)
1.09 (0.45, 2.63)
Remote
0.71 (0.18, 2.75)
0.56 (0.18, 1.75)
Very remote
0.43 (0.11, 1.61)
0.90 (0.32, 2.50)
Inner regional
Reference group
Reference group
Maternal mental health contact b
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Yes
0.75 (0.43, 1.32)
1.29 (0.79, 2.11)
No
Reference group
Reference group
Child has disability
Characteristic
DFV exposure adjusted hazard ratios a (95% CI)
No DFV exposure adjusted hazard ratios a (95% CI)
Yes
2.13 (1.17, 3.88)
1.99 (1.19, 3.32)
No
Reference group
Reference group
Notes: a Adjusted for characteristics listed in table.
b Mother had a mental health diagnosis in HMDC or MHIS records that occurred prior to the child’s mental health contact.
c Bold text denotes statistically significant estimates where the 95 per cent CIs did not include the null value.
Appendix D:
Adjusted hazard ratios and 95 per cent confidence intervals for the risk associated with DFV exposure on specific mental health diagnosis groups stratified by Aboriginal and Torres Strait Islander status
The tables below provide the adjusted hazard ratios and 95 per cent confidence intervals (CIs) for the risk associated with DFV exposure on specific mental health diagnosis groups (relating to Figures 8 and 9 in the report) for Aboriginal and Torres Strait Islander children and non-Aboriginal and Torres Strait Islander children. Individual models were run for each group. The first 10 tables provide information on Aboriginal and Torres Strait Islander children and the last 10 tables provide information on non-Aboriginal and Torres Strait Islander children. Adjustments were made for sex, early gestation (<37 weeks), mother’s age at birth, father’s age at birth, maternal marital status at birth, SES, residential remoteness, disability and maternal mental health contact. Bolded text in the tables denotes statistically significant estimates where the 95 per cent CIs did not include the null value.
Aboriginal and Torres Strait Islander children
Mental health contact with no diagnosis recorded
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
1.45 (1.34, 1.57)
No
Reference group
Other mental illness-related contacts
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
1.07 (0.77, 1.51)
No
Reference group
Intentional self-harm
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
1.67 (1.31, 2.15)
No
Reference group
Substance use disorder
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
1.85 (1.52, 2.25)
No
Reference group
Psychological development disorder
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
1.10 (0.95, 1.27)
No
Reference group
Depressive disorder
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
1.30 (1.00, 1.70)
No
Reference group
Anxiety
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
1.40 (1.25, 1.58)
No
Reference group
Schizophrenia and psychoses
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
1.33 (1.09, 1.61)
No
Reference group
Personality disorder
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
1.71 (0.96, 3.03)
No
Reference group
Organic disorder
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
1.68 (1.02, 2.76)
No
Reference group
Non-Aboriginal and Torres Strait Islander children
Mental health contact with no diagnosis recorded
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
1.56 (1.39, 1.75)
No
Reference group
Other mental illness-related contacts
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
1.35 (0.90, 2.03)
No
Reference group
Intentional self-harm
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
1.30 (0.90, 1.88)
No
Reference group
Substance use disorder
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
2.48 (1.52, 4.05)
No
Reference group
Psychological development disorder
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
1.22 (1.02, 1.45)
No
Reference group
Depressive disorder
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
1.36 (0.99, 1.87)
No
Reference group
Anxiety disorder
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
1.51 (1.31, 1.75)
No
Reference group
Schizophrenia and psychoses
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
1.42 (1.09, 1.86)
No
Reference group
Personality disorder
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
1.66 (0.95, 2.89)
No
Reference group
Organic disorder
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
0.99 (0.55, 1.77)
No
Reference group
Appendix E:
Adjusted hazard ratios and 95 per cent confidence intervals for the risk associated with DFV exposure on specific mental health diagnosis groups stratified by disability status
The tables below provide the adjusted hazard ratios and 95 per cent confidence intervals for the risk associated with DFV exposure on specific mental health diagnosis groups (relating to Figures 10 and 11 in the report) for children with disability and children with no disability. Individual models were run for each group. The first 10 tables provide information on children with disability and the last 10 tables provide information on children with no disability. Adjustments were made for Aboriginal and Torres Strait Islander status, sex, early gestation (<37 weeks), mother’s age at birth, father’s age at birth, maternal marital status at birth, SES, residential remoteness and maternal mental health contact. Bolded text in the table denotes statistically significant estimates where the 95 per cent CIs did not include the null value.
Child with disability
Mental health contact with no diagnosis recorded
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
1.59 (1.44, 1.77)
No
Reference group
Other mental illness-related contacts
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
1.72 (1.55, 1.91)
No
Reference group
Intentional self-harm
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
1.73 (1.56, 1.92)
No
Reference group
Substance use disorder
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
1.72 (1.56, 1.91)
No
Reference group
Psychological development disorder
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
1.53 (1.38, 1.71)
No
Reference group
Depressive disorder
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
1.72 (1.55, 1.91)
No
Reference group
Anxiety disorder
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
1.63 (1.47, 1.81)
No
Reference group
Schizophrenia and psychoses
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
1.71 (1.54, 1.89)
No
Reference group
Personality disorder
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
1.74 (1.57, 1.93)
No
Reference group
Organic disorder
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
1.73 (1.57, 1.92)
No
Reference group
Child with no disability
Mental health contact with no diagnosis recorded
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
1.88 (1.78, 1.98)
No
Reference group
DFV exposure
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
2.03 (1.93, 2.14)
No
Reference group
Intentional self-harm
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
2.02 (1.92, 2.13)
No
Reference group
Substance use disorder
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
2.02 (1.92, 2.13)
No
Reference group
Psychological development disorder
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
1.93 (1.83, 2.04)
No
Reference group
Depressive disorder
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
2.02 (1.91, 2.12)
No
Reference group
Anxiety disorder
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
1.92 (1.82, 2.03)
No
Reference group
Schizophrenia and psychoses
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
2.00 (1.90, 2.11)
No
Reference group
Personality disorder
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
2.05 (1.94, 2.16)
No
Reference group
Organic disorder
DFV exposure
Adjusted hazard ratio (95% CI)
Yes
2.05 (1.94, 2.16)
No
Reference group
Dr Carol Orr
Research Fellow, The School of Population and Global Health,
The University of Western Australia
Scott Sims
Biostatistician, The School of Population and Global Health,
The University of Western Australia
Professor Colleen Fisher
Head of School, The School of Population and Global Health,
The University of Western Australia
Associate Professor Melissa O’Donnell
Deputy Director, Australian Centre for Child Protection,
The University of South Australia
Professor David Preen
Chair in Public Health, The School of Population and Global Health,
The University of Western Australia
Associate Professor Rebecca Glauert
Principal Research Fellow, The School of Population and Global Health,
The University of Western Australia
Professor Helen Milroy
Stan Perron Professor Child and Adolescent Psychiatry Perth Children’s Hospital and
The University of Western Australia
Dr Shae Garwood
Manager, Research, Advocacy & Prevention Innovation & Strategy,
Anglicare WA
Research Report
Issue 10 | July 2022
ANROWS acknowledgement
This material was produced with funding from the Australian Government and the Australian state and territory governments. Australia’s National Research Organisation for Women’s Safety (ANROWS) gratefully acknowledges the financial and other support it has received from these governments, without which this work would not have been possible. The findings and views reported in this paper are those of the authors and cannot be attributed to the Australian Government, or any Australian state or territory government.
ANROWS Acknowledgement of Country
ANROWS acknowledges the Traditional Owners of the land across Australia on which we work and live. We pay our respects to Aboriginal and Torres Strait Islander Elders past, present and future, and we value Aboriginal and Torres Strait Islander histories, cultures and knowledge. We are committed to standing and working with Aboriginal and Torres Strait Islander peoples, honouring the truths set out in the Warawarni-gu Guma Statement.
Peer review process
The quality of ANROWS publications is ensured through a rigorous peer review process that is consistent with the principles of the Committee on Publication Ethics (COPE) Ethical Guidelines for Peer Review. This report has been assessed by at least two peer reviewers with relevant academic expertise.
© ANROWS 2022
With the exception of the ANROWS branding, content provided by third parties, and any material protected by a trademark, all material presented in this publication is licensed under a Creative Commons Attribution-NonCommercial 3.0 Australia (CC BY-NC 3.0 AU) licence.
![]()
The full licence terms are available at creativecommons.org/licenses/by-nc/3.0/au/legalcode
Published by
Australia’s National Research Organisation for Women’s Safety Limited (ANROWS)
PO Box Q389, Queen Victoria Building, NSW 1230 | www.anrows.org.au | Phone +61 2 8374 4000
ABN 67 162 349 171
ISBN: 978-1-922645-34-0 (paperback)
ISBN: 978-1-922645-35-7 (PDF)
Please note that there is the potential for minor revisions of this report.
Please check the online version at www.anrows.org.au for any amendment.
This report addresses work covered in the ANROWS research project RP.20.05 “Investigating the mental health of children exposed to domestic and family violence through the use of linked police and health records”. Please consult the ANROWS website for more information on this project.
ANROWS research contributes to the six National Outcomes of the National Plan to Reduce Violence against Women and their Children 2010–2022. This research addresses National Plan Outcome 4: Services meet the needs of women and their children experiencing violence.
Suggested citation:
Orr, C ., Sims, S., Fisher, C., O’Donnell, M., Preen, D., Glauert, R., Milroy, H., & Garwood, S. (2022). Investigating the mental health of children exposed to domestic and family violence through the use of linked police and health records (Research report, 10/2022). ANROWS.
The University of Western Australia
35 Stirling Hwy
Crawley WA 6009
Author acknowledgement
The authors would like to thank the Linkage, Data Outputs and Research Data Services teams at the Western Australian Data Linkage Branch, in particular the Data Custodians of the Midwives Notification System, Hospital Morbidity Data System, Mental Health Information System, Birth Registration, Death Registration, IDEA Database, Western Australia Register of Developmental Anomalies, Department of Communities – Child Protection and Family Support data, and the Western Australia Police Force. We would also like to thank Wungening Aboriginal Corporation and our community and consumer representative groups. We extend our gratitude to the people of Western Australia for the use of their de-identified administrative data.
This report does not necessarily reflect the views of the government departments involved in this research and any errors of omission or commission are the responsibility of the researchers.
Acknowledgement of lived experiences of violence
ANROWS acknowledges the lives and experiences of the women and children affected by domestic, family and sexual violence who are represented in this report. We recognise the individual stories of courage, hope and resilience that form the basis of ANROWS research.
ANROWS acknowledges that children and young people living in homes where domestic and family violence (DFV) is present are not simply “exposed” to DFV – they are experiencing it. There are no circumstances in which children and young people are exposed to DFV and are not also being impacted by this violence. Therefore, ANROWS will always default to using “experienced DFV” instead of “were exposed to DFV” or “witnessed DFV”. This language aligns with the National Plan to End Violence Against Women and Children (due for finalisation in 2022), which recognises that children experience DFV as victims in their own right, and also seeks to honour the voices of victims and survivors who have felt minimised, erased or unacknowledged as childhood survivors.
Please note that in this report, the authors have chosen to use the term “exposed to DFV”, and have provided a rationale for this choice in the “Definitions and key concepts” section.
Caution: Some people may find parts of this content confronting or distressing. Recommended support services include 1800RESPECT (1800 737 732), Lifeline (13 11 14) and, for Aboriginal and Torres Strait Islander people, 13YARN (13 92 76).
Acronyms
| Acronym | Definition |
|---|---|
| ABS | Australian Bureau of Statistics |
| AEDC | Australian Early Development Census |
| AIFS | Australian Institute of Family Studies |
| AIHW | Australian Institute of Health and Welfare |
| ANROWS | Australia’s National Research Organisation for Women’s Safety |
| ARIA | Accessibility/Remoteness Index of Australia |
| CALD | Culturally and linguistically diverse |
| CI | Confidence interval |
| DSM-5 | Diagnostic and Statistical Manual of Mental Disorders (Fifth Edition) |
| DFV | Domestic and family violence |
| EDDC | Emergency Department Data Collection |
| HMDC | Hospital Morbidity Data Collection |
| HPA axis | Hypothalamic-pituitary-adrenal axis |
| ICD | International Classifications of Disease |
| ICD-9 | International Classifications of Disease Ninth Edition |
| ICD-10AM | International Classifications of Disease 10th Edition Australian Modification |
| IDEA | Intellectual Disability Exploring Answers |
| IMS | Incident Management System |
| MHIS | Mental Health Information System |
| PTSD | Post-traumatic stress disorder |
| RANZCP | Royal Australian and New Zealand College of Psychiatrists |
| SD | Standard deviation |
| SAS | Statistical Analysis System |
| SEIFA | Socioeconomic Indexes for Areas |
| SES | Socioeconomic status |
| SNAICC | Secretariat of National Aboriginal and Islander Child Care |
| UN | United Nations |
| UNICEF | United Nations Children’s Fund |
| VIF | Variance inflation factors |
| WARDA | Western Australian Register of Developmental Anomalies |
| WHO | World Health Organization |
Definitions and concepts
| Concept | Definition |
|---|---|
| Domestic and | Domestic and family violence (DFV) refers to the threat of, or acts of, violence or abuse of a physical, non-physical and/or sexual nature between people who are currently or have previously been in an intimate relationship (Council of Australian Governments, 2011). The central component of DFV is an ongoing pattern of behaviour aimed at controlling a person through fear by use of violent and/or threatening behaviour (Council of Australian Governments, 2011). The acts can be both criminal and |
| Women subjected | Debate exists in regard to the use of the terms “victim” and/or “survivor”. Due to the stigma attached, those living with DFV frequently object to the use of either term (Papendick et al., 2017). As this report uses population linked administrative data, the individual journey of those abused, whether they have started the recovery process or not, and their preference for the use of the term “victim” and/or “survivor” is unknown. Therefore, the term “subjected to DFV” is used throughout this report to describe a woman who has been abused by a man in the context of DFV. |
| Identification of DFV | This report captures DFV perpetrated by men against women. While men can also be victims of DFV perpetrated by a partner of the same or different sex (AIHW, 2018b), DFV is a gendered act that is disproportionately perpetrated by men against women (European Institute for Gender Inequality, 2017; World Health Organization [WHO], 2014). Recognising the gendered patterns of DFV does not negate the experiences of men who are subjected to DFV. It does, however, acknowledge the need to address the issue through a gendered lens. Therefore, in the context of this report, “DFV” refers to DFV perpetrated by men against women. |
| Perpetrator | The men who commit acts of DFV are referred to as “perpetrators”. “Perpetrator” is the term used in the National Outcome Standards for Perpetrator Interventions (National Outcome Standards; Council of Australian Governments, 2015) to describe men who commit DFV against women. While the phrase “men who use violence” is preferred by some (Heward-Belle et al., 2019) because it labels the behaviour rather than the person (Council of Australian Governments, 2015), the term “perpetrator” reinforces the serious nature of DFV. The term includes all men who commit one or more identified acts of DFV. |
| Child | The term “child/children” will be used to capture those under the age of 18 as used in the Children and Community Services Act 2004 (WA). |
| Exposure to DFV | Within the literature there is a lack of common terminology and definitions of children exposed to DFV, despite this issue being acknowledged more than 30 years ago (Fantuzzo & Lindquist, 1989). DFV literature often uses the terms “witnessed” or “exposed to” and at times they are used interchangeably (Berg et al., 2020; Howarth et al., 2016; Kitzman et al., 2003; Spilsbury et al., 2008). The term “witness” is restrictive in the context of DFV. Far from being passive observers, children experience DFV with all of their senses (Devaney, 2015). Moreover, the dichotomy of whether a child observed or overheard violence or not is too simplistic (Holden, 2003). The child may not always observe DFV; the abuse may be psychological and controlling behaviour by the perpetrator and not physically visible to the child, but they are still aware that the abuse is happening (Överlien & Hydén 2009; Swanston et al., 2014). Holden (2003) arguesthat the term “exposed to” is more inclusive of the different types of experiences of the child and does not assume that the child observed the DFV. Holden developed a taxonomy of exposure that is separated into 10 discrete categories (see Table 1). The taxonomy ranges from the child being actively involved in the DFV to the child being ostensibly unaware of it. In this report the term “exposure to DFV” will be used to ensure the capture of the child’s full experience, the scope of which is defined in |
| International Classification of Disease codes | International Classification of Disease (ICD) codes are standardised medical classification codes authorised by the World Health Organization (WHO) for the classification of diseases, injuries, health encounters, social circumstances, external causes of injury or diseases, and inpatient procedures in morbidity (health) settings. The ICD classification is used globally. Some countries, however, have modified it to better suit their needs. Within Australia, the current ICD codes have been amended to suit Australian needs and are known as the ICD-10 Australian Modification (ICD-10-AM). |
| Aboriginal and Torres Strait Islander | The data used in this report contained a variable that identified a combined Aboriginal and Torres Strait Islander status (see Christensen et al., 2014). Therefore, in this report, the term “Aboriginal and Torres Strait Islander” is used in preference to “Indigenous” or “Aboriginal”. |
| Culturally and linguistically diverse | There is considerable inconsistency in how culturally and linguistically diverse (CALD) status is defined within Australia (Pham et al., 2021). CALD can often include those born overseas, those having a parent born overseas, those whose main language spoken at home is not English, and particular religious affiliations (Australian Institute of Health and Welfare [AIHW], 2018a; Pham, 2021). The term “CALD” in this report will include those children with one or both parents born overseas, including the United Kingdom and New Zealand (AIHW, 2018a). |
| Disability | As a concept, disability is complex, dynamic, multidimensional and contested (WHO, 2011a). The term “disability” has divergent meanings with no national or international consensus on how it is defined. In the study contained in this report, a child was defined as having disability if they had a diagnosis for autism, intellectual disability, Down syndrome, cerebral palsy or birth defect. This definition of disability has been used in previous research (e.g. Maclean, Sims et al., 2017). However, the definition of disability used in this report is narrower than that captured in the Australian Bureau of Statistics (ABS; 2016a) due to limitations in the data. |
| Ecological framework | The ecological model was the conceptual framework for the study and informed data analysis. The model was introduced in the 1970s by Urie Bronfenbrenner (1977) to explain how the interactive environment affects a child’s growth and development. While the ecological model was originally used to explain children’s growth and development, an ecological approach to public health issues, such as DFV, has become a more distinctive feature of prevention and promotion in contemporary public health (Richard et al., 2011). The model is a prominent explanatory framework used by the WHO to understand the interplay of personal, situational and socio-cultural factors that influence violence against women (Ellsberg & Heise, 2005; WHO, 2022). |
| Mental health | The WHO (2018) defines mental health as the state of wellbeing in which an individual realises his or her own abilities, can cope with the normal stresses of life, can work productively and fruitfully, and is able to make a contribution to his or her community (WHO, 2018). |
| Internalising behaviours | Internalising behaviours are described as “inner-directed and generating distress in the individual” (Forns et al., 2018, p. 519). Types of internalising behaviours include anxiety, dysphoria and depression. |
| Externalising behaviours | Externalising behaviours are a group of behaviour problems that are “outer-directed generating discomfort and conflict in the surrounding environment” (Forns et al., 2018, p. 519). These behaviours include substance misuse, impulsivity, aggressiveness and disruptiveness. |
| Mental health service contact | An instance of contact or service provision by an agency to an individual which was recorded in the administrative data of the agency. |
| Mental health services | The collective term used in this report to represent the “agency” encompassing |
Table 1: A taxonomy of children’s exposure to domestic violence: Type of exposure (adapted from Holden, 2003, p. 152)
| Type of exposure | Definition | Examples |
|---|---|---|
| Exposed prenatally | Real or imagined effects of DFV on the developing foetus | Foetus assaulted in utero; pregnant mother lived in terror; mothers perceived that the DFV during pregnancy had affected their foetus |
| Intervenes | The child verbally or physically attempts to stop the assault | Asks parents to stop; attempts to defend mother |
| Victimised | The child is verbally or physically assaulted during an incident | Child intentionally injured, accidentally hit by a thrown object, etc. |
| Participates | The child is forced to or “voluntarily” joins in the assaults | Coerced to participate; used as spy; joins in taunting mother |
| Eyewitness | The child directly observes the assault | Watches assault or is present to hear verbal abuse |
| Overhears | The child hears, though does not see, the assault | Hears yelling, threats or breaking of objects |
| Observes the initial effects | The child sees some of the immediate consequences of the assault | Sees bruises or injuries; police; ambulance; damaged property; intense emotions |
| Experiences the aftermath | The child faces changes in their life as a consequence of the assault | Experiences maternal depression; change in parenting; separation from father; relocation |
| Hears about it | The child is told or overhears conversations about the assault | Learns of the assault from mother, sibling, relative or someone else |
| Ostensibly unaware | The child does not know of the assault, according to the source | Assault occurred away from home or while child was away; or occurred when mother believed child was asleep |
Executive summary
Background
Existing literature highlights that exposure to domestic and family violence (DFV) is associated with poorer mental health in childhood (Carter et al., 2020; Gartland et al., 2021; Herrenkohl et al., 2008; Orr, Fisher, Preen et al., 2020). However, the literature is limited by the predominant use of studies focused on a short period of time with little account given to the mental health impacts that may occur over time. Existing research has also focused on the grouping of mental health issues into internalising and externalising behaviours (Vu et al., 2016) which can restrict targeted interventions.
Additionally, there is a need to conduct research in an Australian context given the disparity in rates of both exposure to DFV (Australian Bureau of Statistics [ABS], 2016b; Orr, Preen et al., 2019) and mental illness (Al-Yaman, 2017) for Aboriginal and Torres Strait Islander children. Furthermore, Australia has a long history of migration (Collins, 2013). The most recent Australian Census (ABS, 2021a) reported that 62 per cent of Western Australians have one or both parents born overseas. Evidence is lacking on the outcomes of children who are exposed to DFV and culturally and linguistically diverse (CALD). Additionally, within Australia, 8 per cent of children under 15 have disability (ABS, 2019). The greater dependency of children with disability on carers and family support and the time spent in the family home are thought to place the child at greater risk of DFV exposure (Baldry et al., 2006). The effects of DFV exposure on children withdisability remain poorly understood (Dababnah et al., 2018).
Aim and objectives
The aim of this research was to identify the mental health service use and diagnoses of children exposed to DFV in Western Australia between 1987 and 2016.
The specific objectives were to:
1. Examine the mental health service use and trajectories of children exposed to DFV and ascertain the differences in sociodemographic characteristics and service use between exposed and non-exposed children.
2a. Identify mental health diagnosis types for children exposed to DFV compared to non-exposed children.
2b. Identify key sociodemographic and clinical characteristics predictive of mental health diagnosis and diagnosis subtypes of children with known DFV.
3. Examine differences in mental health service use and diagnosis types in Aboriginal and Torres Strait Islander children and non-Aboriginal and Torres Strait Islander children who are exposed to DFV as well as other sub-populations of children, including those from CALD backgrounds and children with disability, who are exposed to DFV.
Methods
This study comprised a population-based retrospective cohort study of children born in Western Australia between 1987 and 2010 who were exposed to DFV. Exposure to DFV was initially identified in the Western Australia Police Force Information Management System (IMS) when a child’s mother was identified (in Western Australia) as being subjected to DFV from 2004 to the end of 2008, a male perpetrator was charged for the offence and a domestic relationship indicator was recorded. There were 15,598 children born to mothers who were identified as victims of DFV in the Western Australia Police Force IMS. The children were firstly matched in a ratio of 1:3 to a non-DFV-exposed cohort of children based on month of birth, socioeconomic status (SES), Aboriginal and Torres Strait Islander status, and sex. Due to the hidden nature of DFV we also examined non-exposed children for any maternal DFV hospitalisations by interrogating the Western Australian hospitalrecords of their mothers from 1979 to 2016 (inclusive) using International Classification of Diseases (ICD) codes (WHO, 2011b). We found that 4,442 originally “non-exposed” children had a mother who had a hospitalisation indicating DFV. The children exposed to DFV were then restricted to those who were between the ages of 0 and 18 when the identified DFV occurred. This approach resulted in an exposed cohort of 16,356 and a non-exposed cohort of 41,996.
Aboriginal and Torres Strait Islander children were identified by the Western Australian Data Linkage Branch derived Aboriginal status flag. Disability was identified from three sources: 1) the child was recorded in the Western Australian Register of Developmental Anomalies (WARDA) datasets as having a birth defect or cerebral palsy; 2) intellectual disability was captured in the Intellectual Disability Exploring Answers (IDEA) database; or 3) ICD codes were used to identify disability in Hospital Morbidity Data Collection (HMDC) records. CALD children were identified from the WA Registry of Births, Deaths and Marriages where one or both parents were born overseas.
Mental health service use was defined as a child having had any mental illness-related diagnosis across the HMDC, Mental Health Information System (MHIS) and Emergency Department Data Collection (EDDC) datasets during the follow-up period. Children were followed until they reached 18 years of age, date of death or until the end of follow-up period in 2017, whichever came first. Only a child’s first mental illness-related contact after DFV (across the three data collections) was considered for modelling purposes relating to overall service contact.
Mental health diagnosis was identified across the three data collections (HMDC, EDDC and MHIS) utilising ICD codes. The diagnoses were categorised into 10 main groupings: organic disorder, substance use disorder, schizophrenia and psychoses, depressive disorder, anxiety disorder, personality disorder, psychological development disorder, intentional self-harm, other mental illness-related contacts, and mental health contact with no diagnosis recorded.
Multiple approaches to statistical analysis were undertaken.
Results
Children exposed to DFV had a statistically significant 49 per cent increased risk of mental health service contact when compared with non-exposed children. On average the children were exposed to DFV when aged 6.5 years, however, the children were, on average, aged 12.5 years at mental health service contact. Almost half of children exposed to DFV had a mother with a mental health contact (45%) – this was more than double the proportion seen in non-exposed children (21%).
Over time, children exposed to DFV had a 79 per cent chance of having a mental health contact by age 18, whereas for children not exposed to DFV, the chance of having a mental health service contact was 16 per cent by age 18.
Children exposed to DFV had a higher risk of having a diagnosis in eight of the 10 mental health subcategories compared to their non-exposed peers. This ranged from a 19 per cent increased risk in psychological development disorders (which include behavioural and emotional disorders) to a 99 per cent increased risk in substance use disorder. Only the categories “organic disorder” (including cerebral dysfunction) and “other mental illness-related contacts” showed no significant risk increase for children exposed to DFV when compared to non-exposed children.
Aboriginal and Torres Strait Islander children were overrepresented in our exposed cohort when compared to the state of Western Australia. According to the 2016 Census (ABS, 2018c), only 7 per cent of people under 18 in Western Australia were Aboriginal and Torres Strait Islander compared to 62 per cent of children in our exposed group. Possible reasons as to why Aboriginal and Torres Strait Islander children were overrepresented in this cohort are explored in subsequent sections discussing the study’s findings and its strengths and limitations. For Aboriginal and Torres Strait Islander children exposed to DFV, being born to a mother aged under 30 was associated with a decreased risk of mental health service contact of 18 per cent to 25 per cent, compared to those with an older mother. However, for non-exposed Aboriginal and Torres Strait Islander children, maternal age was not associated with mental health service contact.
For children with disability who were exposed to DFV, being born pre-term was associated with a 23 per cent increased risk of mental health service contact when compared to DFV-exposed children born at term. However, being born early was not a risk for mental health service contact in children with disability who were not exposed to DFV.
Due to limitations in the data, outcomes for CALD children were unable to be investigated.
Strengths and limitations
The main strength of the research was the use of population-level administrative data, linked across multiple agencies, at both the child and parent level to investigate the mental health of children exposed to DFV. The use of linked police and hospital data to identify DFV exposure enabled investigations of high-risk groups not captured in previous mental health research.
While the use of linked administrative data provides many advantages, there are some limitations that should be noted. The children identified as exposed to DFV in this report were only recognised because of the mother’s involvement in police or hospital services. As such, the data may be subject to selection bias, capturing mainly physical cases of DFV, and may underestimate the impact of DFV exposure on children’s mental health outcomes due to the fact that not all children exposed to DFV were captured. It is therefore likely that the estimates presented in this report are conservative estimates of the association between DFV and the mental health of children exposed to DFV.
Furthermore, Aboriginal and Torres Strait Islander children were overrepresented in the cohort. This could be, in part, due to the police records of DFV requiring a charge to be made against the man; there is evidence to suggest that the likelihood of being charged for DFV is increased by a variety of socioeconomic and demographic characteristics, such as Aboriginal status (Cunneen, 2010; Jeffries & Bond, 2015). Additionally, DFV was identified in maternal hospital records where Aboriginal and Torres Strait Islander women are overrepresented (Orr, Preen et al., 2019).
The capture of mental illness in children was identified by public and private hospitalisations, emergency department (ED) attendance and public outpatient mental health services. Many children with mental illness will not be identified in these data.
Implications for policy and practice
DFV exposure is associated with an increased risk of mental health service contact and diagnosis of mental illness. Early intervention is required. Many children exposed to DFV are not engaged in mental health services until years after the exposure. Additionally, the findings add further support for the need for a dedicated standalone national response and strategy for the mental health of children exposed to DFV (Australian Government, 2021).
Children exposed to DFV often live with complex issues such as maternal mental illness and disability. Therefore, services to support these children must be well resourced and holistically focused with collaborative, multidisciplinary teams and cross-agency collaboration that provides continuity of care for children and their families with multiple and complex issues.
To support children and families, it is important that mental health clinicians are aware of trauma, including DFV exposure, during childhood. Clinicians need to have knowledge of DFV and its implications for mental health as well as the ability to appropriately and safely respond to children exposed to DFV (McTavish et al., 2016). These skills need to be taught to clinicians during their training and offered as ongoing professional development to enable clinicians to stay abreast of contemporary developments. At present DFV training is not part of the mandatory suite of training across Western Australian health services. A national approach should be taken to ensure that all registered and non-registered staff within public, private and NGO health services are provided with DFV training.
Aboriginal and Torres Strait Islander peoples were overrepresented in the exposed cohort. Such overrepresentation reaffirms calls from Aboriginal and Torres Strait Islander communities that Aboriginal and Torres Strait Islander peoples should receive sufficient investment to develop policies and programs to support Aboriginal and Torres Strait Islander children.
Children exposed to DFV are not engaged in mental health services until years after exposure. To best support children exposed to DFV, early intervention is required. These children and their families are in contact with multiple agencies that may include education, health, police and child protection, and each provides a potential point of intervention. As such, it is imperative that these agencies, along with children’s mental health services, are embedded in, and part of, a broader collaborative, multiagency and multidisciplinary response to DFV, and are adapted to “fit” with the existing local response to DFV and avoid unwarranted duplication of services.
To support service engagement and reduce the re-traumatisation of children exposed to DFV, service responses must be trauma-informed and culturally responsive and secure.
Exposure to DFV is associated with an increased risk of mental health disorders in children. Our findings highlight the importance of the continuation of collective prevention efforts nationally and in each jurisdiction to reduce and eradicate DFV.
Directions for future research
There is a substantial period of time between children’s exposure to DFV and their contact with mental health services. Early access to mental health services is important for children as it can reduce the long-term impact of mental illness (MacDonald et al., 2018). Therefore, it is imperative that future research investigates factors associated with delay in service contact for children exposed to DFV as a priority.
It is acknowledged that children with mental health issues are more likely to have mental health issues in adulthood (Kessler et al., 2005; Ravens-Sieberer et al., 2015). Future research is needed to investigate the mental health of the children exposed to DFV into their adulthood. As young people with complex needs are at greater risk of “falling thorough the gaps” in care transition to adult services (Singh, 2009), attention to those exposed to DFV is needed.
There is a need for research driven by Aboriginal and Torres Strait Islander peoples on the mental health of Aboriginal and Torres Strait Islander children given the disproportionate exposure to DFV of these children. The findings contained in this report have the potential to be a stepping stone from which a holistic, culturally appropriate program of research can be developed.
To gain a greater understanding of the effect exposure to DFV has on children’s mental health, further research is required utilising multiple sources of linked data to identify both DFV and mental illness. The linked data should be complemented by combining data from population-based surveys, longitudinal surveys and social indicators (Hertzman & Williams, 2009). This multiple source approach would largely overcome the limitations of using each source separately and benefit from the strengths of each.
Conclusion
Findings from this research have shown that exposure to DFV in childhood is associated with an increased risk of mental health service contact and mental health diagnosis during childhood. The use of population-level linked administrative data has enabled the identification of sociodemographic characteristics that are associated with mental health service contact and diagnosis categories in children exposed to DFV. Additionally, the longitudinal data has provided a picture of mental health service contact over time for Western Australian children exposed to DFV. The research also offers new insights into the impact DFV has on Aboriginal and Torres Strait Islander children and children with disability.
Introduction
This report outlines the findings of a retrospective cohort study that used linked de-identified administrative data. The aim of the study was to identify the mental health outcomes of children born in Western Australia who were exposed to domestic and family violence (DFV).
Context for research
Domestic and family violence in Australia
It is difficult to accurately identify the extent of DFV in the Australian population. By their nature DFV incidents often occur at home or in other private spaces – “behind closed doors” – and are often concealed and denied by both the perpetrator and those subjected to the violence (Australian Institute of Health and Welfare [AIHW], 2018b; Phillips & Vandenbroek, 2014). The ability of data sources to measure DFV is dependent on the victim’s perception of DFV, their willingness to disclose and/or how the incident is reported (Australian Bureau of Statistics [ABS], 2017a). Global estimates of DFV suggest that almost 33 per cent of women who have been in an intimate partner relationship have experienced physical or sexual violence by an intimate partner in their lifetime (World Health Organisation [WHO], 2020a). Within Australia, DFV perpetrated by a current or former intimate partner is a widespread issue with a lifetime prevalence of 25 per cent(ABS, 2017a). The Australian Personal Safety Survey reports data on women who have been subject to DFV perpetrated by a partner in the previous 12 months. Rates of DFV have remained relatively stable over the past decade, with a slight increase in the latest (2016) survey report: 1.5 per cent of the population were subjected to DFV in 2005 and 2012, increasing to 1.7 per cent in 2016 (ABS, 2017a). DFV occurs at high rates among Aboriginal and Torres Strait Islander women (ABS, 2016b), with 10 per cent of Aboriginal and Torres Strait Islander women informing the 2015 National Aboriginal and Torres Strait Islander Social Survey that they had been victims of DFV by an intimate partner or a family member in the preceding 12 months (ABS, 2016b).
Aboriginal and Torres Strait Islander peoples hold distinctive rights as Australia’s First Peoples, set out in international law (Australian Human Rights Commission, 2015). Additionally, in 2009, Australia gave its formal support to the United Nations Declaration on the Rights of Indigenous People. However, despite these distinctive rights and as a result of colonisation and systemic racism, Aboriginal and Torres Strait Islander communities are considered among the most vulnerable groups in Australia (Australian Human Rights Commission, 2015). The National Plan to Reduce Violence against Women and their Children 2010–2022 (Council of Australian Governments, 2011) acknowledges the disproportionate rates of DFV experienced by Aboriginal and Torres Strait Islander women as a national priority. DFV is not part of traditional Aboriginal and Torres Strait Islander cultures (Blagg et al., 2020; Our Watch, 2018; Wilson et al.,2017). The disproportionate rates largely stem from deep and complex issues around dispossession and intergenerational trauma resulting from the legacy of colonisation, including systemic racism and forced removal of children (Secretariat of National Aboriginal and Islander Child Care [SNAICC], 2017). As part of this study, we explored rates of DFV and mental health disorders among both Aboriginal and Torres Strait Islander women and children and non-Indigenous women and children. In understanding the rates at which different groups experience DFV and mental ill health, research can better inform recommendations for future policy and practice including resource distribution and future research priorities.
Help-seeking by women
The most recent Australian Personal Safety Survey highlighted that around half of women (46%) who are subjected to DFV do not disclose the abuse (ABS, 2017a). A multitude of reasons have been identified: stigma, fear, lack of a safe place to disclose (García-Moreno et al., 2005; Keeling & Fisher, 2015), or believing they can deal with it themselves or that it is not serious enough to seek help (ABS, 2017a). There is also fear of child removal, a particular concern for Aboriginal and Torres Strait Islander women (Australia’s National Research Organisation for Women’s Safety [ANROWS], 2020a). Of the Australian women who do seek assistance, 53 per cent reportedly seek help from a health professional (33% from a general practitioner and 20% from another health professional) and 17 per cent from police (ABS, 2017a).
Children’s exposure to DFV
Children’s exposure to DFV is a prominent human rights issue. The United Nations Convention on the Rights of the Child (United Nations General Assembly, 1989) states that children have a universal right to live free from all forms of violence, including exposure to DFV. As a signatory to this Convention, Australia has international obligations to protect children from exposure to DFV, including acting to prohibit, prevent and respond to DFV through legislative, judicial, social and educational measures. The most recent report to the UN Committee on the Rights of the Child (Australian Human Rights Commission, 2018) on Australia’s implementation of children’s rights recommended the Australian Government increases prevention measures and responses to DFV that address its distinct impacts on children.
Domestic and family violence exposure and child mental health
Due to the hidden nature of DFV and the stigma attached, it is difficult to ascertain the prevalence of children’s exposure to DFV. The Australian Personal Safety Survey (ABS, 2017a) reported that 11 per cent of adult respondents had witnessed violence against their mother by their mother’s partner before the age of 15. Additionally, 49 per cent of the women identified in the survey data as being assaulted by their current partner reported that they had children in their care at the time, with the child hearing or seeing the violence (ABS, 2017a). Research by Indermaur (2001) has suggested that one in four young Australians (12 to 20 years) have been exposed to at least one incident of DFV against their mother or carer. This figure rises to 42 per cent among Aboriginal young people (12 to 20 years; Indermaur, 2001).
Exposure to DFV in childhood has been associated with poor mental health (e.g. Hultmann et al., 2020; Vu et al., 2016). However, much of the literature is from outside of Australia with little account given to the impacts that may occur over time, and more comprehensive evidence is needed. The use of longitudinal linked administrative data provides a means to gain a greater understanding of the long-term impact of DFV exposure on children’s mental health. Poor mental health is a public health concern, and it is estimated that one in seven Australian children aged 4 to 17 years (Goodsell et al., 2017) and almost one in four Aboriginal children aged 5 to 10 years (Shepherd et al., 2017) have a mental health disorder.
Call for research
Authors of this report undertook a “priority setting partnership” process involving those with lived experience, support people and DFV service providers (Fisher et al., 2016) in order to identify community priorities for DFV research. The partnership highlighted that researching the outcomes of children exposed to DFV was a top priority. Additionally, a recent Australian Government report (AIHW, 2018b) highlighted that there are limited data available on the experiences of children exposed to DFV and noted that data sources such as police data and longitudinal data would contribute to a more comprehensive picture of those exposed and subjected to DFV. Additionally, Australia’s National Research Agenda to Reduce Violence against Women and their Children: ANRA 2020–2022 (ANROWS, 2020b) highlights the need to investigate the short- and long-term emotional and psychological impacts of DFV on children as a priority.Furthermore, the National Agreement on Closing the Gap (Commonwealth of Australia. Department of the Prime Minister and Cabinet, 2021) highlights a reduction in incidents of DFV for Aboriginal and Torres Strait Islander families as a key target and highlights the need to explore data development to measure and report the impact of DFV on children.
Study setting
Western Australia is a geographically large state within Australia covering 2.5 million square kilometres. In the 2016 Australian Census the population of Western Australia was almost 2.5 million, with 1.9 million (76%) people residing in the Greater Perth area (ABS, 2021a), an area of almost 6,500 square kilometres. The Western Australian population has a median age of 36 years (ABS, 2017b), with 23 per cent of the population comprised of children 0 to 18 years of age (ABS, 2017c), and 3 per cent of the population is Aboriginal and Torres Strait Islander (ABS, 2021a). A quarter of Aboriginal and Torres Strait Islander peoples in Western Australia reside in very remote locations, with 40 per cent living in major cities. This is in contrast to 80 per cent of non-Aboriginal and Torres Strait Islander Western Australians who live in major cities (ABS, 2017d). The most recently available data has shown the Western Australian population to be representativeof the Australian national population on key sociodemographic, health and economic indicators (Clark et al., 2010).
Aim and objectives
Aim
The aim of this research was to identify the mental health service use and diagnoses of children exposed to DFV in Western Australia between 1987 and 2016.
Objectives
The specific objectives were to:
1. Examine the mental health service use and trajectories of children exposed to DFV and ascertain the differences in sociodemographic characteristics and service use between exposed and non-exposed children.
2a. Identify the mental health diagnosis types for children exposed to DFV compared to non-exposed children.
2b. Identify key sociodemographic and clinical characteristics predictive of mental health diagnosis and diagnosis subtypes of children with known DFV.
3. Examine differences in mental health service use and diagnosis types in Aboriginal and Torres Strait Islander children and non-Aboriginal and Torres Strait Islander children who are exposed to DFV as well as other sub-populations of children, including those from CALD backgrounds and children with disability, who are exposed to DFV.
Structure of this report
This report begins with a review of existing literature, followed by a description of the methodology utilised. The key findings are then presented and are followed by a discussion that provides some interpretation of these findings in relation to the existing literature. The report concludes with the implications of the findings of the study for policy and practice.
State of knowledge review
A state of knowledge review was undertaken to situate the current study among the literature that focuses on children’s exposure to DFV with attention to the factors that impact their mental health.
Review methodology
This state of knowledge review was undertaken as a narrative literature review, an approach used to review and critique available evidence on a given topic or field. Narrative literature reviews are useful in providing a comprehensive overview of the topic and highlighting gaps in existing literature.
To complete this review a number of relevant databases were searched including:
- CINAHL
- Cochrane Library
- JSTOR
- Global Health via Ovid
- MEDLINE via PubMed
- SAGE
- ProQuest 5000
- PsycINFO
- Web of Science
Multiple combinations of keywords to source pertinent information were included: intimate, domestic, gender, family, violence, child, mental health, psychiatric, development, and exposure. As the literature on the outcomes of children exposed to DFV is relatively new, no year limit was set in publication searches. Research that was not published in English was excluded. The references listed in each of the sourced materials were scanned for additional relevant sources. Online searches were used to search for relevant government and non-government organisation publications and additional “grey literature”.
The final materials included in this review were original research, grey literature and unpublished reports.
The impact of DFV exposure
While many studies have investigated the impact of DFV on women, it is only in recent years that significant steps have been made to understand the impact of DFV exposure on children (Kuhlman et al., 2012), with children often referred to as “forgotten victims” (e.g. Reif & Jaffe, 2019; UNICEF, 2006).
Stress response
DFV is considered to be one of the most prevalent stressors children can experience (Margolin & Gordis, 2000), with significant evidence that environmental stressors play a major role in modifying physical and psychological health (e.g. Bair Merritt et al., 2012; Bradley & Dinan, 2010; Juruena et al., 2020). The biological mechanisms linking stress to ill-health, however, are not fully understood, but emerging literature points to a central role of the hypothalamic–pituitary–adrenal axis (HPA axis) function (Juruena et al., 2020; Margolin & Gordis, 2000). The HPA axis is an essential stress response system that enables appropriate response to stressors. While this stress response is vital to adapt to everyday stressors, chronic activation due to exposure to stressful events can challenge physiological response systems, increasing the risk for physical and psychological ill-health (Cohen et al., 2007; Juruena et al., 2020; Kiecolt-Glaser& Glaser, 2005; Mueller & Tronick, 2019).
Mental health
Existing literature has acknowledged that children exposed to DFV may experience delays in cognitive and emotional development (Antle et al., 2010; Mueller & Tronick, 2019) and an increased risk of mental illness (Carter et al., 2020; Herrenkohl et al., 2008; Huang et al., 2021; Kennedy et al., 2010; Kimball, 2016; Orr, Fisher, Preen et al., 2020). An Australian prospective pregnancy cohort study (Gartland et al., 2021) examined the mental health of children exposed to DFV and found that by 10 years of age, they were twice as likely to have anxiety as non-exposed children. Outside of Australia, a study by Olaya and colleagues (2010) captured an older range of children (8 to 17 years) attending a public mental health centre in Spain, and found that children exposed to DFV were twice as likely to have depression than non-exposed children. Similarly, Huang and colleagues’ (2021) longitudinal study of the Fragile Families and Child Well-being Study ofover 200,000 children in the United States also found higher levels of depression in children who were exposed to DFV. Their study identified DFV exposure in children under 4 years of age and followed them in five waves until the children were 15 years old. Previous longitudinal research undertaken by the authors of the current report (Orr, Fisher, Preen et al., 2020) found that Western Australian children aged 0 to 18 who were exposed to DFV before the age of 5 were three times more likely to be hospitalised during childhood for mental health disorders than non-exposed children. The mental health hospitalisations were predominately for mental and behavioural disorders due to acute stress reaction and adjustment disorders, the use of alcohol, major depressive disorder, and mental and behavioural disorders due to the use of volatile solvents.
The majority of the available literature investigating the impact of DFV on children’s mental health groups the behaviours into two distinct categories: internalising and externalising behaviours. Internalising behaviours include depression, somatic or physiological complaints, anxiety, withdrawal, suicidal ideations, eating disorders and phobias. Externalising refers to the outward expression of harmful behaviours such as aggression, hyperactivity and disobedience that affect the external environment. A meta-analysis of 60, mainly cross-sectional, studies by Evans and colleagues (2008) found an association between DFV exposure and an increased likelihood of both internalising and externalising behaviours. A more recent meta-analysis of 74 qualitative studies by Vu and colleagues (2016) also reported an increased likelihood of internalising and externalising behaviours in children exposed to DFV. However, their study went further and investigated thelong-term impact of exposure to DFV on children. They found that the association of DFV exposure and internalising and externalising problems increased over time. The authors highlight that children newly exposed to DFV may display no internalising or externalising behaviours and be thought of as being “resilient” after the exposure. However, they suggest that there may be a “sleeper effect” and the true impact on the child may not manifest for many years after the exposure.
Kernic and colleagues (2003) carried out a study with children (n=167) aged 2 to 17 in the United States whose mothers had been identified in police or court records as being subjected to DFV. They used Achenbach’s Child Behavior Checklist (Achenbach, 1991) to investigate the internalising and externalising behaviours of children exposed to DFV compared to a standardised normative sample (n=2,736) representative of the United States population. They reported that children exposed to DFV had a 60 per cent increase in risk of externalising behaviour compared to the standardised sample. However, they reported a non-significant increase for internalising behaviours compared to the standardised sample. Similarly, Campbell and colleagues’ (2013) retrospective cohort study of children with a recent child protection services investigation and DFV in the preceding 12 months found no significantly increased risk of internalising problems in the children exposedto DFV. However, they reported an 88 per cent increase in risk of externalising behaviours in children exposed to DFV six years after their recruitment in the study. The studies by Kernic et al. (2003) and Campbell et al. (2013) relied on parental reporting of children’s issues, like much of the literature investigating this area. However, the internalising problems may not be visible to the parents. A recent study (Orr et al., 2021) from the current report’s authors overcame the parental reporting issue by using linked administrative data to investigate the early development of children exposed to DFV. The study used Australian Early Development Census (AEDC) data (AEDC, 2022) which contains teacher reporting of children’s early development vulnerability. It was found that young children exposed to DFV were more likely to exhibit internalising behaviours including anxious and fearful behaviour, emotional problems and worrying compared to their non-exposed counterparts.
Olofsson and colleagues’ (2011) study (n=4,947) using data drawn from the Swedish National Health Survey reported that children (aged 0 to 18) exposed to DFV had higher odds of anxiety than non-exposed children. While the odds were significant for both male and female children, differences were apparent between the sexes: girls exposed to DFV had a six-fold increase in odds of anxiety whereas exposed boys had between a two-fold and three-fold increase, depending on their age. It has been postulated that the outcomes for girls may differ as they may be experiencing co-occurring forms of victimisation which have not been taken into account (du Plessis et al., 2015; Seng et al., 2005). These co-occurring abuses can include sexual and physical abuse (Campo, 2015). Moylan and colleagues’ (2010) prospective longitudinal study in the United States found that pre-school children exposed to DFV had higher levels of internalisingand externalising behaviours than non-exposed children. They also reported finding sex differences, with females scoring higher on internalising behaviours, and males higher on externalising behaviours. Moylan et al.’s (2010) study is not alone in finding differences between the sexes: several studies have reported that children exposed to DFV can exhibit different behavioural problems with males more likely to demonstrate externalising behaviours and females more likely to demonstrate internalising behaviours (e.g. du Plessis et al., 2015; Hosokawa & Katsura, 2019; Izaguirre & Calvete, 2018). However, Holmes and colleagues’ (2015) longitudinal study of children (n=1,125) drawn from a national survey of child and adolescent wellbeing in the United States found that among children exposed to DFV, girls were at greater risk of externalising problems than boys. Holmes and colleagues’ findings are not unique, with other researchers reporting higher rates ofexternalising in girls exposed to DFV than boys exposed to DFV (e.g. Bair-Merritt et al., 2015). Indeed, the evidence of sex is equivocal with other studies suggesting no difference or that the difference is a trend that can change with age (Sternberg et al., 2006; Vu et al., 2016).
Exposure to DFV is recognised as a precursor to post-traumatic stress disorder (PTSD) for some children (Boeckel et al., 2017; Margolin & Vickerman, 2007). The stressor criterion for PTSD in the Diagnostic and Statistical Manual of Mental Disorders (Fifth Edition; DSM-5; American Psychiatric Association, 2013) states that a person must have experienced or witnessed a traumatic event, or learned that the traumatic event occurred to a close family member. The DSM-5 stressor criterion for PTSD describes experiences commonly reported in relation to children’s exposure to DFV. Concerns have been raised (Margolin & Vickerman, 2007) that PTSD in children exposed to DFV may be misdiagnosed as another childhood condition, such as hyperactivity, depression or anxiety, due to the fact that psychological health assessments may be made without knowledge of the traumatic incident(s), namely DFV.
While PTSD is included in the DSM-5 as a diagnosable condition, growing research into the effects of trauma on child development has expanded, leading to growing calls from psychologists to include developmental trauma as a diagnostic condition (Abrams, 2021). The lack of inclusion of developmental trauma in current classifications has been argued to result in a lack of either diagnosis or assistance through mental health services. It can also result in misdiagnosis such as attention deficit disorder resulting in treatments more likely to be behavioural and medical interventions rather than trauma-focused therapies.
Burden of mental illness in children
It is estimated that one in seven Australian children aged 4 to 17 (Goodsell et al., 2017) and almost one in four Aboriginal children aged 5 to 10 (Shepherd et al., 2017) have a mental health disorder. Mental health disorders are a leading cause of disease burden in children (AIHW, 2020a). The Young Minds Matter Survey, the latest survey of child and adolescent wellbeing in Australia (Lawrence et al., 2015), reported that 43 per cent of children with a depressive disorder had severe impairment of daily living functioning. This impairment has been highlighted by Lawrence and colleagues (2019) who found that children with mental health disorders are more likely to have poor school attendance compared to their peers. Regular attendance at school is acknowledged as a crucial component of engagement in schooling and a key prerequisite for academic success (Hancock et al., 2017). Furthermore, it is accepted that mental illnessin childhood is associated with a range of poor longitudinal outcomes such as mental illness in adulthood, including mood and anxiety disorders (Nock et al., 2007; Reef et al., 2010) and substance abuse (Fergusson et al., 2007; Nock et al., 2007). Additionally, research has highlighted that mental health disorders in childhood increase the likelihood of criminal offending in adulthood (Anderson et al., 2015).
At a societal level, the economic burden of mental health disorders is substantial. Around $10.6 billion was spent on mental health services in 2018–19 (AIHW, 2021a). Child and adolescent mental health services are costly, with an average of $2,366 per patient per day (AIHW, 2021a).
Sociodemographic characteristics
Maternal mental health
It is acknowledged that women who are subjected to DFV are more likely to have mental illness than those not subjected to DFV (Karakurt et al., 2014; Langdon et al., 2014; Vilariño et al., 2018). A substantial body of evidence suggests that maternal mental illness negatively impacts children’s mental health (Barker et al., 2011; Korhonen et al., 2012; Leis et al., 2014). It is thought that maternal mental illness can impact parenting capacity (Royal Australian and New Zealand College of Psychiatrists [RANZCP], 2016; Smith, 2004); however, it has been acknowledged that the impact will vary by type of mental illness, its duration and its severity (AIHW, 2020a; Reupert et al., 2012). Maternal mental health plays a key role in children’s outcomes: in addition to the challenges surrounding parental mental illness, children exposed to parental mental illness are more likely to experience adversities compared with their non-exposed counterparts (Abel et al.,2019). It has been acknowledged that evidence-based early intervention for maternal mental illness can improve mental health outcomes for children (RANZCP, 2016).
Disability
While the effects of DFV on children’s outcomes are starting to become clearer, the effects on children with disability remain poorly understood (Dababnah et al., 2018; Robinson et al., 2020). Within Australia, 8 per cent of children under 15 years have disability (ABS, 2019). The greater dependency of children with disability on carers and family support and the time spent in the family home are thought to place the child at greater risk of DFV exposure (Baldry et al., 2006). The association between DFV exposure and intellectual disability is complex. Children exposed to DFV in utero are more likely to be born early and with a low birth weight, both of which increase the risk of intellectual disability (Bailey, 2010; Dababnah et al., 2018). Additionally, being subjected to DFV in pregnancy has been correlated with congenital malformations (Hansen et al., 2000; Orr et al., 2022; Ortega-García et al., 2013). Exposure to DFV in utero has also beenassociated with lower IQ scores in children (Huth-Bocks et al., 2001; Koenen et al., 2003; Ybarra et al., 2007), poorer cognitive ability (Orr et al., 2021; Udo et al., 2016) and developmental delays (Dababnah et al., 2018; Udo et al., 2016).
Culturally and linguistically diverse status
Australia has a long history of migration (Collins, 2013). The most recent Australian Census (ABS, 2021a) reported that 62 per cent of Western Australians have one or both parents born overseas. The evidence as to whether prevalence of DFV is higher or lower in CALD women compared to Australian-born women is equivocal (Cox, 2015; Ghafournia & Easteal, 2018). CALD women’s experiences of DFV are often exacerbated through the intersectional nature of forms of oppression, such as racism; changed and changing gender and family roles (Fisher, 2013); and social factors including social isolation (Carline & Easteal, 2014) and lack of awareness of available services (Ghafournia & Easteal, 2018).
Concurrently, evidence is lacking on the outcomes of children who are exposed to DFV and born to CALD parents. This may be due to those from CALD backgrounds not being identified in samples or underrepresented within research.
The most recent Young Minds Matter Survey (Lawrence et al., 2015) in Australia reported mental illness to be less common in children with both carers born overseas (5%) than those with both carers born in Australia (14%). However, findings in this area are equivocal with Minas and colleagues (2013) reporting similar levels of mental illness in children of migrant parents and children of Australian-born parents.
Child maltreatment
Children exposed to DFV are at increased risk for child maltreatment (Herrenkhol et al., 2008; Orr, Fisher et al., 2019), with a concomitant three-fold increased risk of poorer mental health outcomes than their non-abused peers (Maclean et al., 2019). Child maltreatment is generally considered to be behaviour towards a child which has a risk of causing physical or emotional harm from physical abuse, sexual abuse, emotional abuse and/or neglect (Australian Institute of Family Studies [AIFS], 2018), with maltreatment significantly contributing to child mortality and morbidity (Chen et al., 2016; Gilbert et al., 2009; Segal et al., 2021). Chronic stress from the trauma is thought to impact the child’s brain which can result in health problems (National Scientific Council on the Developing Child, 2012). In recent years children’s exposure to DFV has been acknowledged as a type of maltreatment (AIFS, 2018; Graham-Bermann, 2011; Richards, 2011).However, differences exist between state and federal definitions within Australia. The Commonwealth Family Law Act 1975 recognises that exposure to DFV is a form of child abuse – specifically, psychological harm. The Act defines exposure as occurring “if the child sees or hears family violence or otherwise experiences the effects of family violence” (pt I, s 4AB). The Western Australian Children and Community Services Act 2004 widened its definition of emotional abuse, in 2016, to include children’s exposure to DFV. They use the definition from the Restraining Orders Act 1997 (WA). Exposure in this context is defined by the child seeing or hearing the DFV or witnessing physical injuries resulting from DFV. Historically, mothers subjected to DFV have been blamed for not maintaining the safety of their children. However, this is rightfully changing with a growing focus on perpetratoraccountability including the development of policies and practice in child protection on how to respond to DFV (e.g. Government of Western Australia, 2015).
While it is widely cited that there is a considerable overlap between DFV and other types of child maltreatment (e.g. Gracia et al., 2018; Herrenkohl et al., 2008), the extent of this overlap varies significantly in the literature. This may be due in part to robust estimates of any association being difficult to confirm due to the variability in the definitions of child maltreatment, DFV and exposure within the literature. That being said, from a review of 10 studies presenting prevalence of the co-occurrence of DFV with other forms of child maltreatment, Bidarra and colleagues (2016) estimated the prevalence to be between 12 per cent and 70 per cent. Previous research (Orr, Fisher et al., 2019) on Western Australian children (n=524,534) born in a 20-year period found that 41 per cent of children whose mothers were hospitalised for DFV were known to child protection services. Given the high level of overlap among types of maltreatment and links tomultiple poor outcomes (e.g. Maclean, Taylor et al., 2017; Mills et al., 2012) it is difficult to isolate to the effect of a single maltreatment type on a specific outcome.
Socioeconomic status
Despite DFV occurring across all economic strata, low socioeconomic status (SES) has been acknowledged as a risk factor for women subjected to DFV (Orr, Preen et al., 2019; Orr, Fisher, Preen et al., 2020; Reichel, 2017). Low SES is also associated with mental health disorders in childhood, with the most recent national survey of Australian children and young people reporting higher prevalence of mental health disorders in children from low SES than in those residing in higher SES areas (Lawrence et al., 2015).
Aboriginal and Torres Strait Islander children
Based on data from the 2014–15 National Aboriginal and Torres Strait Islander Social Survey (ABS, 2016b), Aboriginal and Torres Strait Islander women experience high rates of DFV. As a result, Aboriginal and Torres Strait Islander children may be more likely to live in homes where violence is present than non-Aboriginal and Torres Strait Islander children. The National Plan to Reduce Violence against Women and their Children 2010–2022 (Council of Australian Governments, 2011) acknowledges the disproportionate rates of DFV and children’s exposure to it as a national priority.
Research indicates that Aboriginal and Torres Strait Islander children are more likely to have poorer mental health than their non-Aboriginal and Torres Strait Islander peers (AIHW, 2018c; Al-Yaman, 2017). The disparity in mental health is the result of cultural genocide, colonisation and racism (Calma et al., 2017; Marmot, 2011; Shepherd et al., 2017). The mental health of Aboriginal and Torres Strait Islander children is a priority in the national agreement between the Australian Government and the Coalition of Aboriginal and Torres Strait Islander Peak Organisations in their commitment to “close the gap” (Commonwealth of Australia. Department of the Prime Minister and Cabinet, 2021) between the outcomes for Aboriginal and Torres Strait Islander and non-Aboriginal and Torres Strait Islander children. Research specific to Aboriginal and Torres Strait Islander children’s experiences of DFV and mental illness is lacking, and it is an area in need ofinvestigation.
Resilience
It is important to note that not all children exposed to DFV will have negative outcomes. Some children who experience adverse events in childhood adapt well and show no maladjustment in their psychological development (Masten, 2001). Children who do not develop negative outcomes and adapt successfully when exposed to adverse circumstances are considered resilient (Howell, 2011). Resilience is a dynamic construct, changing in response to external and internal events and conditions (Herrman et al., 2011; Masten, 2011). It has been described as an individual’s adaptation to manage or cope with significant adversity, risk or stress, which may result in an increased capacity to respond to future adversity (Herrman et al., 2011; Lemerle & Stewart, 2011; Luthar et al., 2000). It is widely accepted that resilience is not only derived from individual personal characteristics but also from external circumstances such as social and cultural determinants(Cicchetti & Valentino, 2006; Study of Environment on Aboriginal Resilience and Child Health Investigators, 2010). The socio-ecological model (Bronfenbrenner, 1977) has been used in this report to identify factors across internal and external systems that influence resilience (Henderson et al., 2016; Howell, 2011). However, as highlighted earlier in this section there may be a “sleeper effect” and the true impact on the child may not manifest for many years after the exposure (Vu et al., 2016).
Using linked administrative data for research on children exposed to DFV
Much use has already been made of the large linked administrative databases in Western Australia to investigate outcomes of children’s adverse childhood experiences, including maltreatment and incarcerated parents (e.g. Bell et al., 2018; Hafekost et al., 2017; Maclean et al., 2020). However, the use of linked administrative data to investigate the impact of DFV on children is emerging. Linked administrative datasets provide numerous research benefits. Firstly, such data are based on the whole population which reduces selection biases that are present in most DFV exposure research, such as small samples drawn from refuges and other specialist services. Specialist services are often used for sampling for a plethora of reasons including difficulty in identifying children exposed to DFV, maintaining the safety of the child and their family, and ensuring that the children have appropriate mental health support when recalling their experiences (Btoush &Campbell, 2003; Fraga, 2016; Paavilainen et al., 2014). Utilising linked administrative data overcomes many of these issues. Furthermore, we are able to investigate important groups such as Aboriginal and Torres Strait Islander children and children with disability utilising administrative data because, as noted, it includes the whole population. Linked administrative data also provides access to important factors that can impact on the outcomes of children and be adjusted for in analysis, such as SES, mother’s marital status and mother’s mental health.
Conclusion
Exposure to DFV is a significant stressor for Australian children. Existing literature highlights that exposure to DFV is associated with poorer mental health in childhood. However, the literature is limited by the predominant use of cross-sectional studies with little account given to the mental health impacts that may occur over time. Existing research has also focused on the grouping of mental health issues into internalising and externalising behaviours which can restrict targeted interventions. Additionally, there is a need to conduct research in an Australian context given the disparity of both exposure to DFV and mental illness for Aboriginal and Torres Strait Islander children. Children exposed to DFV may not present with mental illness for many years. The use of longitudinal linked administrative data provides a clearer understanding of the long-term impact of DFV exposure on children’s mental health and takes into account factors that arelikely to co-occur with DFV exposure that will also impact their mental health. The lack of available evidence to inform best-practice principles for interventions for children exposed to DFV means that current interventions may be sub-optimal, or even inappropriate. This project provides an opportunity to identify areas for targeted and evidence-based interventions and polices by utilising the best possible data.
Methods
The objective of this study was to explore the mental health service use of, and mental health diagnosis associated with, children exposed to DFV. This was achieved via a population-based cohort study using de-identified linked administrative data of children born in Western Australia between 1987 and 2010. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting checklist (von Elm et al., 2008) was used to guide this report.
Conceptual framework
In acknowledgement of the disproportionate levels of violence against women perpetrated by men this study was underpinned by feminist theory (Dobash & Dobash, 1979; Yodanis, 2004). Additionally, a socio-ecological model (see for example Heise, 1998) was adopted as the conceptual framework for this study. Ecological models were introduced in the 1970s by Bronfenbrenner (1977) to explain how the interactive environment affects a child’s growth and development. It was argued that human development is the product of bi-directional interactions (processes) between an individual (person) and the many developmental settings (context) to which the individual is exposed over the life course (time; Bronfenbrenner, 1994). The socio-ecological model has also been used to integrate the array of personal, situational and social factors that interact to gain understandings of DFV (Heise, 1998), with the WHO adopting Heise’s ecological model in their work onDFV (WHO, 2020b). The model is appropriate for the current study as children exposed to DFV are more likely to live with multiple stressors (McGavock & Spratt, 2017) and an ecological framework is a useful approach to consider the complex variables that influence a child’s mental health (D’Andrea & Graham-Bermann, 2017). The model is also able to incorporate both feminist and social science insights.
Data sources
An overview of the data collections and the main variables extracted for the research presented in this report are shown in Table 2.
Table 2: Data collection variables and periods of coverage used in this report
| Dataset | Period of coverage contained in this report | Main variables extracted |
|---|---|---|
| WA Registry of Births, Deaths and Marriages | 1987–2010 | Date of birth (mm/yyyy) Sex Gestation Born in hospital Mother’s age Birth weight |
| Midwives Notification System | 1987–2010 | Date of birth (mm/yyyy) Sex Maternal age Maternal marital status Mother’s previous pregnancies Gestation ARIA a SEIFA b |
| Hospital Morbidity Data Collection (HMDC) | 1970–2016 | Admission date Separation date Age at admission Principal diagnosis External cause codes Additional diagnosis |
| Emergency Department Data Collection (EDDC) | 2002–2016 | Presentation date (mm/yyyy) Principal diagnosis External cause of injury code |
| Mental Health Information System (MHIS) | 1970–2017 | Primary diagnosis Date of birth (mm/yyyy) Age at contact Episode start date Date of contact |
| Department of Communities, Child Protection and Family Support (CPFS) dataset | 1990–2016 | Reason type Reason start date Reason end date Primary nature of concern Period of care start date Period of care end date |
| Western Australian Register of Developmental Anomalies (WARDA) | 1987–2016 | Diagnosis code Major or minor malformation Sex |
| Intellectual Disability Exploring Answers (IDEA) dataset | 1987–2016 | Level of intellectual disability Date of birth (mm/yyyy) Type of disability |
| Western Australia Police Force Incident Management System (IMS) | 2004–2008 | Offence Partner type Children present Location of offence |
Notes: a.Accessibility/Remoteness Index of Australia.
b Socioeconomic Indexes for Areas.
Mental Health Information System
The MHIS has been collecting information since 1966 and includes all records of patients using inpatient and outpatient public mental health services and private inpatient services. Inpatient data are collected from mental health hospital wards and community accommodation support programs. Outpatient information is collected from psychiatric clinics, triage services, community mental health centres, psychiatric day centres and rehabilitation programs. Clinical data that are collected include principal diagnosis, start and end date of the mental illness episode, and the date that the individual utilised mental health services. The diagnosis is coded using ICD codes. The MHIS data also includes demographic details (e.g. age, sex).
Hospital Morbidity Data Collection
The HMDC is a database of information about hospital admissions. It includes summaries of all admission records for both public and private hospital inpatients. Records are structured on a patient’s episode of care, with each record containing information regarding an admission and clinical procedures carried out, discharge and separation from hospital, and demographic information. The diagnosis information includes one principal diagnosis, up to four co-diagnoses, and up to 20 additional diagnoses. The record also contains external cause of injury codes. This information can include place of event and circumstances of the injury. The HMDC has been in operation since 1970 and in that time it has utilised several editions of ICD codes. The ICD-8 was utilised between 1970 and December 1978; the ICD-9 was used between January 1979 and December 1987; the ICD-9-Clinical Modification (ICD-9-CM) was used between January 1988 and June 1999; and theICD-10-Australian Modification (ICD-10-AM) has been used from July 1999 until the present date.
Emergency Department Data Collection
The EDDC includes information on all presentations to emergency departments of public hospitals in Western Australia, as well as emergency department activity in private hospitals under contract with the Western Australian Government. Records in this collection date back to 2002. Information recorded includes primary diagnosis (when applicable), coded per ICD-10-AM, and demographic information including date of birth, sex, Aboriginal and Torres Strait Islander status and country of birth.
Cohort selection
Exposure to DFV was initially identified in children born between 1987 and 2010 (inclusive) whose mother was identified in Western Australia Police Force IMS data from 2004 to the end of 2008 as a victim of DFV where a male perpetrator was charged for the offence and a domestic relationship indicator was recorded. This approach has been used in previous research (Orr, Fisher, Preen et al., 2020; Orr, Fisher, Glauert et al., 2020). The criminal offences included were murder, attempted murder, assault and injury, sexual assault, threatening behaviour and misuse of weapons/explosives. There were 15,598 children born to mothers who were identified as victims of DFV in police data during the period 2004 to 2008 (inclusive). Children were initially individually matched at a ratio of 1:3 (15,598:46,438) to a non-DFV (i.e. non-exposed) cohort of children based on month of birth, SES, Aboriginal and Torres Strait Islander status and sex. Due to the hiddennature of DFV (Francis et al., 2017) we also examined non-exposed children for any maternal DFV hospitalisations by interrogating the hospital records of their mothers from 1979 to 2016 (inclusive) using ICD codes used in previous research (Orr, Preen et al., 2019; Orr, Fisher, Preen et al., 2020). We found that 4,442 originally “non-exposed” children had a mother who was hospitalised for DFV-related injuries. Finally, we identified children in the exposed group who were exposed to DFV between birth and 18 years. This resulted in an exposed cohort of 16,356 and a non-exposed cohort of 41,996 children (Figure 1).
Figure 1: Cohort selection flowchart
Note: a Includes the 4,442 children identified in the original cohort of children whose mother had no police record for DFV victimisation (2004–2008) but had a maternal hospitalisation for DFV.
Data linkage
Data linkage is defined as “the bringing together[,] from two or more different sources, data that relate to the same individual, family, place or event” (Holman et al., 2008, p. 767). Data linkage involves the linkage of administrative (and other) data that are collected by governments and non-government agencies for service delivery and administrative purposes. These data are commonly collected at the population level, can be made available for research and contain rich, detailed information. The linking of data sets from multiple sources can provide greater insights than those generated by single sources (Harron et al., 2017). While population-level administrative data do not capture the level of detail that may be sourced from survey data, linked individual-level administrative data has become an attractive alternative as it provides longitudinal information; is free of biases which typically affect survey data such as recall, response andselection biases, and attrition; and it is comparatively cost-effective as the data are already collected (Jutte et al., 2011; Pearson, 2015). Linked administrative data can provide large sample sizes and detailed data on hard-to-reach populations, such as children exposed to DFV, enabling evidence to be generated with a high level of external validity and applicability for policymaking (Harron et al., 2017).
Data custodians are the gatekeepers of administrative datasets and have a number of rights and responsibilities in relation to the release and access of datasets by researchers (Australian Government, 2018), including ensuring that the research project is of public benefit.
Datasets were linked, for both exposed and non-exposed groups, by the Western Australian Data Linkage Branch using probabilistic linkage (Holman et al., 1999). Data were provided as individual linkable datasets to the report authors, then de-identified and merged using a project-specific encrypted linkage key (Kelman et al., 2002). No identifiable information was received by the researchers involved in this study.
The Western Australia Police Force provided data from their IMS to the Western Australian Data Linkage Branch for women who had been subjected to DFV that resulted in the male perpetrator being charged with an offence. The children of the females subjected to DFV were linked by the Data Linkage Branch using the WA Midwives Notification System.
WA Family Connections System
The WA Family Connections System contains links between individuals who are related, created using information from datasets that identify multiple related people, for example Birth Registrations and Midwives’ Notifications (Glasson et al., 2008). These relationships are usually biological. No information is known about adoptions, including step, local or overseas adoptions; other care arrangements; or divorces. The genealogy held by the Data Linkage Branch includes parents and siblings of people born in Western Australia since 1945. Extended family members (including grandparents, grandchildren, cousins, aunts and uncles) can also be identified (Government of Western Australia Department of Health, 2022). Links are available for people born in Western Australia and their family members who have migrated to Western Australia and had contact with one of the government agencies listed in Table 2. To connect the family members the researchers wereprovided with a separate mapping file that include a “linkage key” for the child matched to a corresponding linkage key for the family member. For this study linkage keys were provided to connect a child with their mother and their father across datasets.
Consent
Administrative data in Western Australia are collected without consent. To ensure confidentiality and ethical practice, strict processes exist for access to linked administrative data. To gain access to data, researchers must adhere to the Data Linkage Branch’s Access and Charging Policy. Researchers are required to discuss potential projects with the data custodian of each database from which they are requesting data and gain their approval to access the data. Aboriginal data sovereignty
affirms the rights of Indigenous peoples to determine the means of collection, access, analysis, interpretation, management, dissemination and re-use of data pertaining to the Indigenous peoples from whom it has been derived, or to whom it relates. (Walter et al., 2021, p. 4)
This project engaged with Aboriginal people and Aboriginal community-controlled organisations (see “Community and consumer involvement” subsection for further detail) about the design and interpretation of the data. Additionally, approval was gained from the Western Australian Aboriginal Health Ethics Committee (WAAHEC), with WAAHEC reviewing the report prior to publication. WAAHEC monitors outputs to ensure that they are ethically sound and culturally appropriate, as well as to ensure benefit to Aboriginal and Torres Strait Islander peoples.
Cohort characteristics
Domestic and family violence exposure
Western Australia Police Force data have a mandatory “domestic flag” variable which has been recorded since the implementation of the Frontline IMS system in 2004. This variable draws on the type of behaviour alleged and the relationship between the parties.
The type of DFV is indicated in police data by the Australian and New Zealand Standard Offence Classification (ABS, 2011a) subdivision level. The DFV types are murder and attempted murder, assault and injury, sexual assault, threatening behaviour, and misuse of weapons/explosives (see Appendix A for further details). The data from IMS made available to the researchers were from 1 January 2004 to 31 December 2008.
HMDC records do not contain a “DFV flag”. Therefore, records of the mothers were searched for ICD codes used in previous studies (Orr, Preen et al., 2019; Orr, Fisher, Preen et al., 2020) that identify DFV (Table 3).
The project is based on the assumption that children in the majority reside with their mother as primary caregiver.
Table 3: ICD codes identifying DFV
| ICD code | Definition | ICD edition |
|---|---|---|
| E960–E969 | Homicide and injury purposely inflicted by other persons | ICD-9 a |
| 995.81 | Adult physical abuse | ICD-9 a |
| V71.5 | Observation following alleged rape or seduction | ICD-9 a |
| E980–E989 | Injury undetermined whether accidentally or purposely inflicted | ICD-9 a |
| V61.1 | Counselling for marital and partner problems | ICD-9 a |
| T74.1 | Physical abuse | ICD-10-AM b |
| T74.2 | Sexual abuse | ICD-10-AM b |
| T74.3 | Psychological abuse | ICD-10-AM b |
| Z04.4 | Examination and observation following alleged rape or seduction Examination of victim or culprit following alleged rape or seduction | ICD-10-AM b |
| X85-Y09 | Assault | ICD-10-AM b |
| Y10-Y34 | Event of undetermined intent | ICD-10-AM b |
| Z63.0 | Problems in relationship with spouse or partner. Discord between partners resulting in severe or prolonged loss of control, in generalisation of hostile or critical feelings or in a persisting atmosphere of severe interpersonal violence (hitting or striking) | ICD-10-AM b |
Notes: a International Classification of Diseases Ninth Edition.
b International Classifications of Disease 10th Edition Australian Modification.
Aboriginal and Torres Strait Islander status
Aboriginal and Torres Strait Islander children were identified by the Western Australian Data Linkage Branch derived Aboriginal status flag. The flag, developed by the Data Linkage Branch in collaboration with the Australian Institute of Health and Welfare (AIHW), is derived by a validated algorithm when an individual is recorded as Aboriginal and/or Torres Strait Islander in Western Australian Government administrative data sets (Christensen et al., 2014).
Disability
Disability was flagged from three sources: first, a record of the child in WARDA datasets as having a birth defect or cerebral palsy, and second, intellectual disability captured in the IDEA database. Third, following consultation with advisors from WARDA, ICD codes were identified (Table 4) that were used to search the child’s HMDC records to further capture disability.
Table 4: ICD codes capturing disability
| Disability description | ICD-9 | ICD-10 |
|---|---|---|
| Intellectual disability | 317–319 | F70–F79 |
| Autism | 299.0 | F84.0, F84.1 |
| Down syndrome | 758.0 | Q90 |
| Cerebral palsy | 343 | G80 |
| Birth defects | 740–759 (excluding 758.0) 243, 246.1, 255.2, 270, 271.3, 272.4, 271.0, 271.1, 271.2, 272.3, 271.8, 272.7, 330.1, 277.5, 271.8, 271.9, 272.7, 277.2, 277.1, 277.4, 277.8, 275.1, 275.3, 275.4, 277, 272.6, 277.6, 277.8, 330.2, 330.4, 330.8, 331.9, 359.0, 359.1, 359.2 | Q00–Q99 (excluding Q90) E03.0, E03.1, E25.0, E25.9, E70–E73.0, E74.0–E74,4, E75, E76, E77, E79.1, E79.8, E79.9, E80.0-E80.5, E83.0, E83.3, E83.5, E84, E88.0, E88.1, E88.8, G31.8, G31.9, G32.8, G71 |
Culturally and linguistically diverse children
We aimed to investigate the mental health service contact and mental health diagnosis by subtypes of CALD children who were exposed to DFV compared with non-CALD children exposed to DFV. However, this was unable to be empirically examined due to limitations in the data.
Socioeconomic status
Neighbourhood-level SES was determined by the Socio-Economic Indexes for Areas (SEIFA) using the Midwives Notification System. The SEIFA score is based on information from the Australian Census about income, education, employment, occupation and housing, and provides a measure of relative SES for the area where a person resides. Five levels of disadvantage were assigned to Census collection districts (~250 households), ranging from 1 (high disadvantage) to 5 (low disadvantage; ABS, 2018a).
Residential remoteness
Residential remoteness was determined by the Accessibility/Remoteness Index of Australia (ARIA), based on the distance of geographic locations from the nearest population centre, ranging from major cities to very remote Australia (ABS, 2018b). Residential remoteness was identified in the Midwives Notification System from collection district, with the smallest spatial unit available equating to approximately 250 households (ABS, 2011b).
Mothers’ mental health service contact
Mothers’ mental health service contact was identified if the mother had a record in the MHIS dataset, which included both public and private inpatient services and public outpatient services for psychiatric care. HMDC records were also searched for mental health admissions. Mothers’ mental health contacts occurring after a child’s first mental health contact were excluded from analysis.
Maternal marital status
Mothers’ marital status was identified in the Midwives Notification System. They were grouped into four categories: married/de facto/widowed, never married, divorced/separated and unknown/not stated.
Parents’ age
Mothers’ age at the child’s birth was identified in the Midwives Notification System and grouped into four categories: under 20 years, 20–29 years, 30–39 years and 40 years and over. Fathers’ age details were also identified in the Midwives Notification System and groups using the same categories as above. Not all children had their father’s age available so a fifth category of “missing age” was added.
Early gestation
Early gestation was identified in the Midwives Notification System. A child born prior to 37 weeks gestation was classified as being born pre-term.
Child protection involvement
Child protection involvement was identified in the Western Australia Department of Communities dataset where a notification had been made regarding concern for the child. A child was deemed to have been in contact with child protection services if they had ever had at least one record of notification, period of care, order, placement or application within the child protection and family support data sets. Child protection involvement was moderately correlated with DFV (> 0.6), which can make it difficult to separate the effects of each risk factor. Using variance inflation factors (VIF) to test for collinearity, child protection involvement and DFV had VIF=1.82, meaning no evidence of collinearity. However, as DFV is a recognised form of child abuse (Richards, 2011), child protection was excluded in analysis due to the conceptual similarities and the challenge of disentangling the effect (Richards, 2011).
Outcomes
The primary study outcomes were childhood mental health service contact and mental illness diagnosis. Children were followed from birth until end of follow-up on 31 December 2017, date of death or the age of 18, whichever came first. Outcomes were examined in the cohort overall and separately in Aboriginal and Torres Strait Islander children and children with disability.
Mental health service use was ascertained by combining records of mental health contacts/discharges and diagnoses across the HMDC, MHIS and EDDC data collections. The primary diagnosis code in HMDC is mandatory; HMDC records used in this study had fully populated primary diagnosis. Population of diagnosis in EDDC is not mandatory, and 68.5 per cent of EDDC records used in this study had principal diagnosis missing. MHIS data had 39.7 per cent of records missing a primary diagnosis. The overall measure of mental health service contact was defined as a child having had any mental illness-related diagnosis (yes/no) in HMDC or EDDC data and/or any recorded contact in MHIS during the follow-up period. Only a child’s first mental illness-related contact after DFV (across the three data collections) was considered for modelling purposes relating to overall service contact.
Mental health diagnosis was captured by utilising ICD codes to identify diagnostic outcomes. These diagnoses were grouped according to mental health types. Mental health diagnoses were categorised into 10 main groupings (Table 5). Self-harm was included in mental health service contact and diagnosis grouping: while self-harm is not a mental illness it is often linked to mental distress. The inclusion of self-harm in mental health service contact is an approach used in previous research (Maclean et al., 2019). It is important to note that children with more than one diagnosis during childhood could be counted in multiple diagnostic groups.
Table 5: Mental illness-related ICD diagnostic codes
| Mental illness group a | ICD-9 codes | ICD-10 codes |
|---|---|---|
| Organic disorder | 290, 293, 294 | F00–F09 |
| Substance use disorder | 292, 304, 305 | F10–F19, F55 |
| Schizophrenia and psychoses | 295, 297, 298 | F20–F29, F30, F31, F32, F33, F34.8, F34.9, F38, F39 |
| Depressive disorder | 296, 300.4, 311 | F32.0, F32.9, F33.0, F34.1 |
| Anxiety disorder | 300, 300.0, 300.2, 300.3, 300.8, 308, 309 | F40–F45, F48, F63.3, F68 |
| Personality disorder | 301 | F60, F61, F62, F68, F69 |
| Psychological development disorder | 299, 307.2, 307.3, 307.6, 307.7 312, 313, 314, 315 | F80–F89, F90–F98 |
| Intentional self-harm | E950–E959 | X60–X84 |
| Other mental illness-related contacts | 300.1, 300.5, 300.6, 300.7, 300.9, 302, 306, 307.0, 307.1, 307.4, 307.5, 307.8, 307.9, 310, 316 | F44, F50–F54, F59, F64, F65, F66, F99 |
| Mental health contact with no diagnosis recorded b | No mental illness-related ICD codes | No mental illness-related ICD codes |
Notes: a Children with more than one diagnosis could be counted in multiple diagnostic groups.
b Comprises children with a mental health contact in MHIS who had no mental health diagnosis and had no other mental health diagnosis identified in HMDC or EDDC data.
Community and consumer involvement
Community and consumer consultation
Prior to the initiation of the project, members of the research team undertook a research priority setting process through a partnership with those with lived experience of DFV, their informal support people and DFV service providers. This priority setting process highlighted that the impact of DFV on children was a priority area for research (Fisher et al., 2016). The researchers also met with the Developmental Pathway Project Community and Consumer Group at the Telethon Kids Institute to gain feedback and comment on the proposed research. Meetings were also held with the Kulunga Aboriginal Research Development Unit (KARDU) at the Telethon Kids Institute, which is involved with building the capacity and development of researchers working on research projects that include a focus on Aboriginal outcomes. Meetings were also held with Ruah Community Services, an organisation providing community DFV services. Additionally, discussions were held with seniorstaff at Aboriginal community-controlled health services within Western Australia. Support for the research was gained from the Wirraka Maya Health Service Aboriginal Corporation and Moorditj Koort Aboriginal Health and Wellness Centre.
Post-initiation project support was provided by the Wungening Aboriginal Corporation to help facilitate a reference group to discuss and interpret report findings prior to publication.
Reference group
In addition to the community and consumer involvement outlined above, this project included three reference groups, the members of which provided feedback and advice on the interpretation of the research results and the implications of key findings for policy and practice. The first reference group was recruited by the WA Health Translation Network and comprised both Aboriginal and non-Aboriginal women with lived experience of DFV and/or mental illness. The second reference group comprised Aboriginal and Torres Strait Islander women with lived experience of DFV who were residing in a refuge service provided by Wungening Aboriginal Corporation. The third reference group was the Linking for Life community and consumer group, members of which have an understanding of using linked administrative data for research.
Statistical analysis
Descriptive analysis was conducted for all variables. Sociodemographic variable groupings were initially assessed for crude associations using Chi-square tests. Multivariate Cox regression was used to estimate the association between DFV and mental health service contact in children, with separate analyses for mental health sub-type groupings and by Aboriginal and Torres Strait Islander status and children with disability. Estimates are presented as adjusted and unadjusted hazard ratios (HR) with Wald 95 per cent confidence intervals (CI). Kaplan-Meier survivor function estimates for all categorical covariates were approximately parallel and hence each adhered to the proportional hazards assumption (Kleinbaum & Klein, 2012). Collinearity of covariates was tested using variance inflation factors where VIF>10 was deemed to be collinear (Vittinghoff et al., 2012). No covariates considered for modelling were collinear based onthese conditions. Models were adjusted for known sociodemographic confounders including sex, Aboriginal and Torres Strait Islander status, gestational period, SEIFA and ARIA. Parental sociodemographic factors were also included in the models as potential predictive variables, such as mother’s age at birth, father’s age at birth, marital status and previous mental health service contact by the mother. Potential predictors known to increase the risk of the outcome were included. Each potential predictor was analysed separately to determine the univariate association with the outcome variable. Results in which the 95 per cent CIs did not include the null value of 1 were considered statistically significant. Time to first mental health-related contact was measured in months from birth. All models were tested for interactions, with no combinations showing significance at the p<0.05 level.
A random assignment of virtual DFV exposure was applied to children not exposed to DFV matched by birth year to account for different cohort follow-up periods in children exposed to DFV and those not exposed. Non-exposed children assigned virtual times to mental health service contact that exceeded their total length of available follow-up were excluded from analysis (n=815).
The predicted number of mental health contacts was calculated to plot the trajectories of children exposed and not exposed to DFV according to different sociodemographic characteristics. Trajectories demonstrated time (in months) from first DFV (“time zero”) until first mental health service contact (or censored at death or once they had reached 18 years of age). All analyses were performed using Statistical Analysis System (SAS) statistical software (version 9.4) using the PHREG and LIFETEST procedures.
To investigate mental health service use over time we used trajectory plots to show the estimated cumulative probability (i.e. chance) of a child experiencing a mental health service contact over time (in years) from their birth until they reached 18 years of age. The trajectories are categorised according to those who had been exposed to DFV and those who were not exposed. These subgroups were further categorised according to a series of sociodemographic characteristics that are associated with higher risk of mental health contacts – specifically sex, SES, disability status and Aboriginal and Torres Strait Islander status. Cumulative probability curves were compared for differences using Gray’s test (Gray, 1988). A Gray’s p-value<0.05 was considered a statistically significant difference.
To identify key sociodemographic characteristics of mental health diagnosis and diagnosis subtypes of children with known DFV we stratified our analysis by DFV exposure. Findings for non-exposed children allow comparison.
Research indicates that Aboriginal and Torres Strait Islander children are at an increased risk of exposure to DFV (ABS, 2016b) and mental illness compared to non-Aboriginal and Torres Strait Islander Australians (AIHW, 2018c). To gain an insight into the characteristics that increase the risk of mental health service contact for Aboriginal and Torres Strait Islander children we stratified our analysis by exposure to DFV. We also examined the risk of having a mental health diagnosis subtype for Aboriginal and Torres Strait Islander children exposed to DFV and Aboriginal and Torres Strait Islander children not exposed to DFV.
To gain an insight into the impact exposure to DFV has on Aboriginal and Torres Strait Islander children we examined the subcategories of mental health of exposed Aboriginal and Torres Strait Islander children compared to non-exposed Aboriginal and Torres Strait Islander children. We also investigated the subcategories of mental health for non-Aboriginal and Torres Strait Islander children exposed to DFV compared to non-exposed, non-Aboriginal and Torres Strait Islander children.
It is acknowledged that children with disability are more likely to have mental illness than children without disability (Emerson & Hatton, 2007; Hebron & Humphrey, 2014; Wadman et al., 2011). To gain an insight into the characteristics that increase the risk of mental health service contact for children with disability we stratified our analysis by disability status. We also examined the subcategories of mental health diagnosis of children with disability exposed to DFV compared to non-exposed children with disability.
Ethics
Ethics approval was gained from the Western Australian Department of Health Human Research Ethics Committee (#2016.60), the Western Australian Aboriginal Health Ethics Committee (#756) and The University of Western Australia Human Research Ethics Committee (RA/4/1/8867).
Results
Cohort sociodemographic characteristics
There were 58,352 children in our cohort, comprising 16,356 (28%) children who were exposed to DFV between birth and 18 years of age, and a non-DFV-exposed comparison group of 41,996 (72%) matched children. Table 6 highlights the characteristics of the children in the cohort.
Aboriginal and Torres Strait Islander children were over-represented in our cohort when compared to the state of Western Australia. According to the 2016 Census (ABS, 2018c), only 7 per cent of people under 18 years in Western Australia were Aboriginal and Torres Strait Islander, compared to 62 per cent of children in our exposed group and 50 per cent in our non-exposed group.
The exposed group also had a higher proportion of being born to teenage mothers (26% versus 15%) and unmarried mothers (31% versus 19%) and having a mother with a mental health disorder (45% versus 21%), compared to the non-exposed children. A higher proportion of children exposed to DFV were from a very remote area (21%) compared to non-exposed children (13%).
Over half of the children exposed to DFV were known to child protection services (53%). This proportion is considerably higher than the 4 per cent seen in the non-exposed group and higher than the national rate of 3 per cent reported by the AIHW (2021b).
A higher proportion of the exposed cohort had a mental health service contact compared to the non-exposed cohort (23% versus 11%).
There was a significant difference (p<0.0001) between the average age of mental health contact for children exposed to DFV (12.5 years) compared to non-exposed children (11.6 years). The average age of DFV exposure in our exposed group was 6.5 years.
Table 6: Sociodemographic information of the cohort
Aboriginal and/or Torres Strait Islander
| Characteristic | Childhood DFV | No recorded childhood DFV | p-value c |
|---|---|---|---|
| Yes | 10,205 (62.4) | 20,919 (49.8) | <0.0001 |
| No | 6,151 (37.6) | 21,077 (50.2) |
Sex
| Characteristic | Childhood DFV | No recorded childhood DFV | p-value c |
|---|---|---|---|
| Female | 7,984 (48.8) | 20,537 (48.9) | 0.346 |
| Male | 8,372 (50.2) | 21,459 (51.1) |
Born prior to 37 weeks gestation
| Characteristic | Childhood DFV | No recorded childhood DFV | p-value c |
|---|---|---|---|
| Yes | 2,324 (14.2) | 4,353 (10.4) | <0.0001 |
| No | 14,032 (85.8) | 37,643 (89.6) |
Mother’s age at birth
| Characteristic | Childhood DFV | No recorded childhood DFV | p-value c |
|---|---|---|---|
| <20 years | 4,205 (25.7) | 6,122 (14.6) | <0.0001 |
| 20–29 years | 9,460 (57.8) | 22,774 (54.2) | |
| 30–39 years | 2,591 (15.8) | 12,478 (29.7) | |
| 40+ years | 100 (0.6) | 622 (1.5) |
Father’s age at birth
| Characteristic | Childhood DFV | No recorded childhood DFV | p-value c |
|---|---|---|---|
| <20 years | 1,313 (8.0) | 2,260 (5.4) | <0.0001 |
| 20–29 years | 6,755 (41.3) | 16,754 (39.9) | |
| 30–39 years | 3,144 (19.2) | 14,703 (35.0) | |
| 40+ years | 590 (3.6) | 2,829 (6.7) | |
| Age missing | 4,554 (27.8) | 5,450 (13.0) |
Maternal marital status at birth
| Characteristic | Childhood DFV | No recorded childhood DFV | p-value c |
|---|---|---|---|
| Married/de facto/widowed | 10,732 (65.6) | 33,300 (79.3) | <0.0001 |
| Never married | 5,129 (31.4) | 7,920 (18.9) | |
| Divorced/separated | 369 (2.3) | 564 (1.3) | |
| Unknown/not stated | 126 (0.8) | 212 (0.5) |
Socioeconomic status
| Characteristic | Childhood DFV | No recorded childhood DFV | p-value c |
|---|---|---|---|
| 1–Most disadvantaged | 8,966 (54.8) | 20,569 (49.0) | <0.0001 |
| 2 | 3,457 (21.1) | 9,549 (22.7) | |
| 3 | 2,236 (13.7) | 6,251 (14.9) | |
| 4 | 1,159 (7.1) | 3,857 (9.2) | |
| 5–Least disadvantaged | 538 (3.3) | 1,760 (4.2) |
Residential remoteness
| Characteristic | Childhood DFV | No recorded childhood DFV | p-value c |
|---|---|---|---|
| Major cities | 7,079 (43.3) | 20,261 (48.3) | <0.0001 |
| Inner regional | 1,485 (9.1) | 4,520 (10.8) | |
| Outer regional | 2,318 (14.2) | 6,725 (16.0) | |
| Remote | 2,047 (12.5) | 5,190 (12.4) | |
| Very remote | 3,427 (21.0) | 5,300 (12.6) |
Mean age (years) of child at exposure to DFV
| Characteristic | Childhood DFV | No recorded childhood DFV | p-value c |
|---|---|---|---|
| 6.5 (SD 4.8) d |
Maternal mental health contact a
| Characteristic | Childhood DFV | No recorded childhood DFV | p-value c |
|---|---|---|---|
| Yes | 7,286 (44.6) | 8,788 (20.9) | <0.0001 |
| No | 9,070 (55.5) | 33,208 (79.1) |
Disability
| Characteristic | Childhood DFV | No recorded childhood DFV | p-value c |
|---|---|---|---|
| Yes | 2,495 (15.3) | 5,071 (12.07) | <0.0001 |
| No | 13,861 (84.8) | 36,925 (87.9) |
Known to child protection services b
| Characteristic | Childhood DFV | No recorded childhood DFV | p-value c |
|---|---|---|---|
| Yes | 8,667 (53.0) | 1,588 (3.8) | <0.0001 |
| No | 7,689 (47.0) | 40,408 (96.2) |
Mental health contact
| Characteristic | Childhood DFV | No recorded childhood DFV | p-value c |
|---|---|---|---|
| Yes | 3,808 (23.3) | 4,602 (11.0) | <0.0001 |
| No | 12,548 (76.7) | 37,394 (89.0) |
Mean age (years) of mental health contact
| Characteristic | Childhood DFV | No recorded childhood DFV | p-value c |
|---|---|---|---|
| 12.5 (SD 3.6) | 11.6 (SD 4.3) | <0.0001 |
Notes: a Mother had a mental health diagnosis in HMDC or MHIS records that occurred prior to the child’s mental health episode.
b Child has a record of notification to department for child protection and family support.
c p-value at 95 per cent level.
d SD= standard deviation.
Sociodemographic groupings may not add to 100 per cent due to rounding.
Risk of mental health service contact and mental health diagnosis in children exposed to DFV
Risk of mental health contact in children exposed to DFV
During their childhood, children exposed to DFV had an unadjusted 70 per cent increased risk of mental health contact compared to non-exposed children over the same period (Table 7). Following model adjustment, we found a statistically significant 49 per cent increased risk of mental health service contact, during childhood, for children exposed to DFV compared with non-exposed children.
Several other characteristics were found to be independently associated with mental health service contact including being Aboriginal and Torres Strait Islander, having disability, having a mother who was divorced or separated at the child’s birth, and being born to a mother over 40 years of age (Table 7).
Table 7: Adjusted and unadjusted risk of mental health service contact in childhood
Aboriginal and/or Torres Strait Islander
| Characteristic | Unadjusted hazard ratios (95% CI) c | Adjusted a hazard ratios (95% CI) |
|---|---|---|
| Yes | 1.49 (1.42, 1.56) d | 1.34 (1.27, 1.42) |
| No | Reference group | Reference group |
Sex
| Characteristic | Unadjusted hazard ratios (95% CI) c | Adjusted a hazard ratios (95% CI) |
|---|---|---|
| Female | 0.97 (0.93, 1.02) | 0.99 (0.95, 1.04) |
| Male | Reference group | Reference group |
Born prior to 37 weeks gestation
| Characteristic | Unadjusted hazard ratios (95% CI) c | Adjusted a hazard ratios (95% CI) |
|---|---|---|
| Yes | 1.36 (1.27, 1.46) | 1.14 (1.07, 1.22) |
| No | Reference group | Reference group |
Mother’s age at birth
| Characteristic | Unadjusted hazard ratios (95% CI) c | Adjusted a hazard ratios (95% CI) |
|---|---|---|
| < 20 years | 1.47 (1.37, 1.57) | 1.04 (0.96, 1.14) |
| 20–29 years | 1.15 (1.08, 1.22) | 0.98 (0.92, 1.05) |
| 30–39 years | Reference group | Reference group |
| 40+ years | 1.39 (1.13, 1.72) | 1.29 (1.04, 1.60) |
Father’s age at birth
| Characteristic | Unadjusted hazard ratios (95% CI) c | Adjusted a hazard ratios (95% CI) |
|---|---|---|
| < 20 years | 1.54 (1.40, 1.70) | 1.11 (0.99, 1.24) |
| 20–29 years | 1.25 (1.18, 1.32) | 1.09 (1.03, 1.17) |
| 30–39 years | Reference group | Reference group |
| 40+ years | 1.27 (1.14, 1.41) | 1.23 (1.10, 1.37) |
| Missing age | 1.75 (1.64, 1.87) | 1.23 (1.14, 1.34) |
Maternal marital status at birth
| Characteristic | Unadjusted hazard ratios (95% CI) c | Adjusted a hazard ratios (95% CI) |
|---|---|---|
| Married/de facto/widowed | Reference group | Reference group |
| Never married | 1.45 (1.38, 1.52) | 1.13 (1.07, 1.20) |
| Divorced/separated | 1.70 (1.45, 1.99) | 1.36 (1.16, 1.60) |
| Unknown/not stated | 2.23 (1.74, 2.86) | 1.76 (1.37, 2.26) |
Socioeconomic status
| Characteristic | Unadjusted hazard ratios (95% CI) c | Adjusted a hazard ratios (95% CI) |
|---|---|---|
| 1–Most disadvantaged | 1.50 (1.31, 1.72) | 1.31 (1.14, 1.51) |
| 2 | 1.32 (1.15, 1.52) | 1.25 (1.08, 1.44) |
| 3 | 1.38 (1.19, 1.59) | 1.31 (1.13, 1.52) |
| 4 | 1.19 (1.02, 1.40) | 1.21 (1.03, 1.42) |
| 5–Least disadvantaged | Reference group | Reference group |
Residential remoteness
| Characteristic | Unadjusted hazard ratios (95% CI) c | Adjusted a hazard ratios (95% CI) |
|---|---|---|
| Major cities | 1.07 (0.98, 1.15) | 1.06 (0.97, 1.14) |
| Inner regional | Reference group | Reference group |
| Outer regional | 1.04 (0.95, 1.15) | 0.96 (0.88, 1.06) |
| Remote | 1.17 (1.06, 1.28) d | 1.00 (0.91, 1.11) |
| Very remote | 1.10 (1.00, 1.20) | 0.81 (0.74, 0.89) |
Maternal mental health contact b
| Characteristic | Unadjusted hazard ratios (95% CI) c | Adjusted a hazard ratios (95% CI) |
|---|---|---|
| Yes | 1.41 (1.35, 1.48) | 1.16 (1.11, 1.22) |
| No | Reference group | Reference group |
DFV during childhood
| Characteristic | Unadjusted hazard ratios (95% CI)c | Adjusted a hazard ratios (95% CI) |
|---|---|---|
| Yes | 1.70 (1.62, 1.78) | 1.49 (1.42, 1.57) |
| No | Reference group | Reference group |
Child has disability
| Characteristic | Unadjusted hazard ratios (95% CI) c | Adjusted a hazard ratios (95% CI) |
|---|---|---|
| Yes | 1.77 (1.67, 1.87) | 1.67 (1.58, 1.77) |
| No | Reference group | Reference group |
Notes: a Multivariate analysis adjusted for all characteristic variables in table.
b Mother had a mental health diagnosis in HMDC, EDDC or MHIS records that occurred prior to the child’s mental health contact.
c CI = confidence interval.
d Bold text denotes statistically significant estimates where the 95 per cent CIs did not include the null value.
Mental health diagnosis in children exposed to DFV
Many children who were using mental health services had no formal mental health diagnosis captured in mental health services or hospital data – specifically, 12 per cent of children exposed to DFV and 6 per cent of non-exposed children. To gain an insight into the impact DFV exposure has on children’s mental health, we investigated 10 subcategories of mental health (Figure 2). Details of adjusted hazard ratios presented can be found in Appendix B.
Following model adjustment, we found that children exposed to DFV had a 19 to 99 per cent higher risk of having a diagnosis in eight of the 10 subcategories compared to their non-exposed peers (Figure 2), with only the categories “organic disorder” and “other mental illness-related contacts” showing no significant risk increase.
As shown in Figure 2, children exposed to DFV had a two-fold increased risk of substance use disorder, a 76 per cent increased risk of personality disorder and a 59 per cent increased risk of self-harm compared to non-exposed children. We also found that children exposed to DFV had a 49 per cent increased risk of anxiety disorder and a 39 per cent increased risk of schizophrenia compared with non-exposed children.
Figure 2: Risk of child with DFV exposure having a mental health subcategory diagnosis compared to non-exposed children
| Mental health subcategory | Adjusted hazard ratios (95% CI) |
|---|---|
| Mental health contact with no diagnosis record | 1.52 (1.42, 1.62) |
| Other mental illness-related contacts | 1.21 (0.94, 1.56) |
| Intentional self-harm | 1.59 (1.30, 1.96) |
| Substance use disorder | 1.99 (1.66, 2.38) |
| Psychological development disorder | 1.19 (1.06, 1.33) |
| Depressive disorder | 1.36 (1.11, 1.66) |
| Anxiety disorder | 1.49 (1.37, 1.63) |
| Schizophrenia and psychoses | 1.39 (1.19, 1.63) |
| Personality disorder | 1.76 (1.18, 2.61) |
| Organic disorder | 1.41 (0.97, 2.04) |
Note: Risk calculated using adjusted hazard ratios. Individual models were run for each subcategory. Models were adjusted for Aboriginal and Torres Strait Islander status, sex, early gestation (<37 weeks), mother’s age at birth, father’s age at birth, maternal marital status at birth, SES, residential remoteness, disability and maternal mental health contact. Error bars denote 95 per cent confidence intervals.S
Characteristics associated with mental health service contact and diagnosis
Characteristics associated with increased risk of mental health service contact
Table 8 shows the results from multivariate modelling examining the association between characteristics and mental health service contact in exposed and non-exposed children.
Aboriginal and Torres Strait Islander children in the exposed group had a 25 per cent increased risk of mental health service contact, while there was a 35 per cent increased risk of mental health service contact in non-exposed Aboriginal and Torres Strait Islander children. For children exposed to DFV, having disability was associated with a 41 per cent significantly increased risk of mental health service contact compared to children exposed to DFV with no disability. However, in non-exposed children with disability a significantly increased risk of 88 per cent was seen when compared to non-exposed children without disability.
In children exposed to DFV, having a mother under 30 years of age was associated with a 16 to 17 per cent reduced risk of mental health service contact when compared to children exposed to DFV born to a mother aged 30 to 39. This is in contrast to the non-exposed children, where being born to a teenage mother increased the risk of mental health service contact by 20 per cent when compared to non-exposed children born to a mother aged 30 to 39. Additionally, for non-exposed children, being born to a mother aged 20 to 29 had no significant impact on risk when compared to non-exposed children born to a mother aged 30 to 39. Maternal mental health contact did not increase the risk of mental health service contact for children exposed to DFV when compared to children exposed to DFV whose mother had no mental health service contact. Conversely, it was associated with a 34 per cent significantly increased risk in non-exposed children when compared tonon-exposed children whose mother had no mental health service contact.
Low SES was associated with an increased risk of mental health service contact in non-exposed children, when compared to least disadvantaged SES children who were not exposed. However, low SES was not associated with mental health service contact in children exposed to DFV when compared to least disadvantaged SES children not exposed to DFV.
Table 8: Risk of mental health service contact in childhood for children exposed to DFV and children not exposed to DFV
Aboriginal and/or Torres Strait Islander
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Yes | 1.25 (1.15, 1.37) c | 1.35 (1.25, 1.45) |
| No | Reference group | Reference group |
Sex
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Female | 1.02 (0.95, 1.10) | 0.98 (0.92, 1.04) |
| Male | Reference group | Reference group |
Born prior to 37 weeks gestation
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Yes | 1.17 (1.06, 1.29) | 1.11 (1.01, 1.22) |
| No | Reference group | Reference group |
Mother’s age at birth
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| <20 years | 0.83 (0.72, 0.95) | 1.20 (1.07, 1.34) |
| 20–29 years | 0.84 (0.75, 0.94) | 1.04 (0.96, 1.13) |
| 30–39 years | Reference group | Reference group |
| 40+ years | 1.26 (0.82, 1.92) | 1.30 (1.01, 1.67) |
Father’s age at birth
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| < 20 years | 1.09 (0.92, 1.29) | 1.09 (0.94, 1.27) |
| 20–29 years | 1.13 (1.01, 1.26) | 1.05 (0.97, 1.14) |
| 30–39 years | Reference group | Reference group |
| 40+ years | 1.31 (1.07, 1.61) | 1.19 (1.04, 1.36) |
| Missing age | 1.23 (1.09, 1.39) | 1.22 (1.10, 1.36) |
Maternal marital status at birth
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Married/de facto/widowed | Reference group | Reference group |
| Never married | 1.05 (0.97, 1.14) | 1.19 (1.10, 1.29) |
| Divorced/separated | 1.11 (0.88, 1.42) | 1.54 (1.25, 1.91) |
| Unknown/not stated | 1.81 (1.27, 2.59) | 1.68 (1.17, 2.39) |
Socioeconomic status
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| 1–Most disadvantaged | 1.06 (0.86, 1.31) | 1.51 (1.25, 1.83) |
| 2 | 1.02 (0.83, 1.27) | 1.43 (1.18, 1.73) |
| 3 | 1.19 (0.96, 1.49) | 1.42 (1.16, 1.73) |
| 4 | 1.05 (0.82, 1.33) | 1.34 (1.09, 1.66) |
| 5–Least disadvantaged | Reference group | Reference group |
Residential remoteness
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Major cities | 1.11 (0.97, 1.27) | 1.02 (0.92, 1.13) |
| Inner regional | Reference group | Reference group |
| Outer regional | 1.00 (0.85, 1.16) | 0.95 (0.84, 1.06) |
| Remote | 1.03 (0.87, 1.20) | 0.98 (0.87, 1.11) |
| Very remote | 0.81 (0.69, 0.94) | 0.81 (0.71, 0.92) |
Maternal mental health contact
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Yes | 0.94 (0.88, 1.02) | 1.34 (1.26, 1.43) |
| No | Reference group | Reference group |
Child has disability
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Yes | 1.41 (1.28, 1.54) | 1.88 (1.74, 2.02) |
| No | Reference group | Reference group |
Notes: a Adjusted for characteristics listed in table.
b Mother had a mental health diagnosis in HMDC or MHIS records that occurred prior to the child’s mental health contact.
c Bold text denotes statistically significant estimates where the 95 per cent CIs did not include the null value.
Characteristics associated with increased risk of mental health subtypes
Characteristics that were associated with an increased risk of mental health subtypes for children exposed to DFV are displayed in Table 9. The table only displays characteristics that were significantly associated with increased risk. The full set of results of all sociodemographic characteristics, stratified by DFV exposure, can be found in Appendix C.
For children exposed to DFV, being Aboriginal and Torres Strait Islander was associated with a significantly increased risk of substance use disorder of 192 per cent. For non-exposed children, being Aboriginal and Torres Strait Islander was correlated with a 360 per cent increased risk of substance use disorder (see Appendix C for all non-exposed results).
Being female was associated with a significantly increased risk of diagnosis in six of the mental health diagnostic subcategories for children exposed to DFV, ranging from a 36 per cent increased risk of anxiety disorder to a significantly increased risk (183%) of depressive disorder. Similarly, non-exposed female children also had a significantly increased risk in the same six subcategories, ranging from 48 per cent for anxiety disorder and personality disorder to 220 per cent for intentional self-harm.
Having disability was associated with a significant increase in the risk of a diagnosis in nine of the 10 mental disorder subcategories for children exposed to DFV. This association ranged from a 31 per cent increase in anxiety disorder to a 180 per cent increase in substance use disorder. Similarly, having disability was associated with an increased risk in seven of the 10 subcategories in non-exposed children, ranging from 61 per cent in anxiety disorder and personality disorder to 228 per cent in psychological development disorder.
Table 9: Association of sociodemographic characteristics on the risk of childhood mental health diagnosis by subcategory in children exposed to DFV
| Sociodemographic characteristics | Anxiety disorder | Psychological development | Substance use disorder | Schizophrenia and psychoses | Intentional self-harm | Depressive disorder | Organic disorder | Personality disorder | Other mental illness-related contacts | Mental health contact with no diagnosis recorded |
|---|---|---|---|---|---|---|---|---|---|---|
| Aboriginal and Torres Strait Islander | 192% Grey shading | |||||||||
| Female | 36% Grey shading | 95% Grey shading | 181% Grey shading | 183% Amber shading | 100% Amber shading | 100% Grey shading | ||||
| Born prior to 37 weeks gestation | 35% Amber shading | 19% Amber shading | ||||||||
| Father’s age at birth 20–29 years | 31% Amber shading | |||||||||
| Father’s age at birth missing a | 45% Amber shading | 89% Amber shading | ||||||||
| Maternal marital status at birth: divorced/separated | 36% Grey shading | |||||||||
| ARIA: major city | 48% Amber shading | |||||||||
| Child has disability | 31% Grey shading | 167% Grey shading | 180% Amber shading | 53% Amber shading | 55% Amber shading | 72% Amber shading | 113% Amber shading | 149% Amber shading | 149% Amber shading |
Notes: a Father’s age at birth missing in Midwives Notification System.
Models were adjusted for Aboriginal and Torres Strait Islander status, sex, early gestation (<37 weeks), mother’s age at birth, father’s
age at birth, maternal marital status at birth, SES, residential remoteness, disability and maternal mental health contact.
Grey shading indicates that the associated risk is lower than that observed in children not exposed to DFV. Amber shading indicates the associated risk is greater than observed in children not exposed to DFV.
Mental health service use and trajectories of children exposed to DFV
Probability of mental health service contact in childhood by DFV exposure
Figure 3 displays the cumulative probability of mental health service contact over time for children exposed to DFV and children not exposed. The cumulative probability of having a mental health service contact was higher for children exposed to DFV, who had a 78.6 per cent chance of having a mental health contact by age 18. For children not exposed to DFV the cumulative probability of having a mental health service contact was 15.9 per cent by age 18.
Figure 3: Cumulative probability of mental health service contact over time by DFV exposure
Note: Differences in cumulative probability between children exposed and not exposed to DFV: Gray’s p-value<0.0001.
Probability of mental health service contact in childhood by sex and DFV exposure
Prior to 15 years of age, male children exposed to DFV had the highest probability of a mental health service contact with 17.5 per cent cumulative probability (Figure 4). However, at the end of follow-up, the cumulative probability of having a mental health service contact was highest in female children exposed to DFV: they had a 30.5 per cent chance of having a mental health service contact by 18 years of age, which is slightly higher than the 28 per cent cumulative probability seen in males at the same time point.
Figure 4: Cumulative probability of mental health service contact over time by exposure status and sex
Notes: Differences in cumulative probability between non-exposed female and non-exposed male: Gray’s p=0.0748.
Differences in cumulative probability between exposed female and exposed male: Gray’s p=0.9367.
Probability of mental health service contact in childhood by SES and DFV exposure
Figure 5 displays the cumulative probability of having a mental health service contact by 18 years of age, stratified by SES and DFV exposure. Due to low counts within the initial quintiles of SES, the categories were collapsed to “lowest 20 per cent disadvantage” (i.e. the lowest 20th percentile of most disadvantaged) and “upper 80 per cent of disadvantage” (i.e. the upper 80th percentile of least disadvantaged). There was minimal difference between the trajectories for lower and upper disadvantage groups, with the most variation observed within the non-exposure group. The cumulative probability of having a mental health service contact by 18 years was 28.7 per cent for those exposed to DFV, irrespective of their SES status.
Figure 5: Cumulative probability of mental health service contact over time by exposure status and socioeconomic status
Notes: Differences in cumulative probability between least and most disadvantaged non-exposed children: Gray’s p<0.0001.
Differences in cumulative probability between least and most disadvantaged children exposed to DFV: Gray’s p=0.8011.
Probability of mental health service contact in childhood by disability status and DFV exposure
The comparison of children with and without disability and their cumulative probability of having a mental health service contact by exposure status is shown in Figure 6. Until age 10, children with disability and no DFV exposure had the highest probability of mental health service contact of all four groups. However, after 10 years of age, children with disability who were exposed to DFV had the highest cumulative probability of a mental health service contact: 36.3 per cent by the time they reach 18.
For children without disability, the cumulative probability of mental health service contact was similar until around age 9, after which point the trajectory increased more rapidly in children exposed to DFV. By age 18, non-exposed children without disability had a 16.3 per cent likelihood of mental health service contact whereas children exposed to DFV without disability had a 27.7 per cent cumulative probability of mental health service contact.
Figure 6: Cumulative probability of mental health service contact over time by exposure status and disability
Notes: Differences in cumulative probability between non-exposed children with disability and without: Gray’s p<0.0001.
Differences in cumulative probability between children exposed to DFV with disability and without: Gray’s p<0.0001.
Probability of mental health service contact in childhood by Aboriginal and Torres Strait Islander status and DFV exposure
Prior to 12 years of age, non-Aboriginal and Torres Strait Islander children exposed to DFV had the highest cumulative probability of mental health service contact: 8.8 per cent of the four groups (Figure 7). However, over time, the cumulative probability of having a mental health service contact is highest for Aboriginal and Torres Strait Islander children exposed to DFV, who had a 31.6 per cent probability of having a mental health service contact by 18. By the end of follow-up, non-Aboriginal and Torres Strait Islander children with no DFV exposure had the lowest cumulative probability of having a mental health service contact (13.2%).
Figure 7: Cumulative probability of mental health service contact over time by exposure status and Aboriginal and Torres Strait Islander status
Notes: Differences in cumulative probability between Aboriginal and Torres Strait Islander children with and without exposure: Gray’s p<0.0001.
Differences in cumulative probability between non-Aboriginal and Torres Strait Islander children with and without exposure: Gray’s p<0.0001.
Aboriginal and Torres Strait Islander children
Characteristics associated with increased risk of mental health service contact in Aboriginal and Torres Strait Islander children
Table 10 displays the characteristics associated with mental health service contact for Aboriginal and Torres Strait Islander children exposed to DFV and Aboriginal and Torres Strait Islander children not exposed to DFV. Accounting for sociodemographic characteristics, Aboriginal and Torres Strait Islander children exposed to DFV who were born pre-term (prior to 37 weeks gestation) were 18 per cent more likely to have a mental health service contact than those born at term. Similar associated increased risk was seen in Aboriginal and Torres Strait Islander children born pre-term but not exposed to DFV.
For Aboriginal and Torres Strait Islander children exposed to DFV, being born to a mother aged under 30 was associated with a decreased risk of mental health service contact of 18 to 25 per cent, compared to those with an older mother. Conversely, maternal age was not associated with mental health service contact for non-exposed Aboriginal and Torres Strait Islander children. Being born to a father aged over 40 was associated with an increased risk of mental health service contact by 68 per cent in Aboriginal and Torres Strait Islander children exposed to DFV, compared with having a younger father. Father’s age was not associated with mental health service contact for Aboriginal and Torres Strait Islander children not exposed to DFV.
Having a mother’s marital status at birth missing or unknown in the Midwives Notification System was associated with an increased risk of mental health service contact of 75 per cent in Aboriginal and Torres Strait Islander children exposed to DFV, compared to those whose mother was married, widowed or in a de facto relationship. A similar risk increase was observed in the non-exposed children. Unlike children exposed to DFV, where no association was found, being born to a mother who was divorced was observed to increase the risk of mental health service contact by 35 per cent in Aboriginal and Torres Strait Islander children not exposed to DFV.
Being born in a major city was associated with an increased risk of mental health service contact for Aboriginal and Torres Strait Islander children exposed to DFV by 37 per cent compared with children exposed to DFV residing in inner regional areas. A 19 per cent increased risk in mental health service contact was observed in the non-exposed Aboriginal and Torres Strait Islander children residing in major cities compared to non-exposed inner regional children. Conversely, for Aboriginal and Torres Strait Islander children not exposed to DFV, residing in a very remote regional area was associated with a 16 per cent decreased risk of mental health service contact compared to those in inner regional areas. However, no significant association was seen in children exposed to DFV residing in a remote area for mental health service contact.
Being born to a mother who had a prior mental health contact was not associated with mental health service contact in children exposed to DFV. However, it was associated with a 10 per cent increase in risk of contact in non-exposed children.
For Aboriginal and Torres Strait Islander children exposed to DFV, having disability was associated with a 28 per cent greater risk of mental health service contact than Aboriginal and Torres Strait Islander children exposed to DFV who do not have disability. However, for non-exposed Aboriginal and Torres Strait Islander children, having disability was associated with a higher risk of 75 per cent, when compared to non-exposed Aboriginal and Torres Strait Islander children without disability.
Table 10: Risk of mental health service contact in childhood for Aboriginal and Torres Strait Islander children with exposure to DFV and without exposure to DFV
Sex
| Characteristic | Exposed to DFV adjusted hazard ratios b (95% CI) | No DFV exposure adjusted hazard ratios (95% CI) |
|---|---|---|
| Female | 0.97 (0.89, 1.06) | 0.93 (0.86, 1.00) |
| Male | Reference group | Reference group |
Born prior to 37 weeks gestation
| Characteristic | Exposed to DFV adjusted hazard ratios b (95% CI) | No DFV exposure adjusted hazard ratios (95% CI) |
|---|---|---|
| Yes | 1.18 (1.05, 1.33) c | 1.14 (1.02, 1.28) |
| No | Reference group | Reference group |
Mother’s age at birth
| Characteristic | Exposed to DFV adjusted hazard ratios b (95% CI) | No DFV exposure adjusted hazard ratios (95% CI) |
|---|---|---|
| <20 years | 0.75 (0.63, 0.88) | 1.10 (0.96, 1.27) |
| 20–29 years | 0.82 (0.71, 0.94) | 0.98 (0.88, 1.10) |
| 30–39 years | Reference group | Reference group |
| 40+ years | 0.85 (0.42, 1.73) | 1.32 (0.90, 1.92) |
Father’s age at birth
| Characteristic | Exposed to DFV adjusted hazard ratios b (95% CI) | No DFV exposure adjusted hazard ratios (95% CI) |
|---|---|---|
| <20 years | 1.08 (0.88, 1.34) | 1.01 (0.85, 1.20) |
| 20–29 years | 1.07 (0.92, 1.24) | 0.96 (0.86, 1.08) |
| 30–39 years | Reference group | Reference group |
| 40+ years | 1.68 (1.30, 2.18) | 1.22 (0.99, 1.49) |
| Missing age | 1.15 (0.99, 1.34) | 1.17 (1.03, 1.32) |
Maternal marital status at birth
| Characteristic | Exposed to DFV adjusted hazard ratios b (95% CI) | No DFV exposure adjusted hazard ratios (95% CI) |
|---|---|---|
| Married/de facto/widowed | Reference group | Reference group |
| Never married | 1.03 (0.93, 1.13) | 1.09 (1.00, 1.20) |
| Divorced/separated | 1.17 (0.86, 1.58) | 1.35 (1.05, 1.75) |
| Unknown/not stated | 1.75 (1.18, 2.61) | 1.74 (1.19, 2.56) |
Socioeconomic status
| Characteristic | Exposed to DFV adjusted hazard ratios b (95% CI) | No DFV exposure adjusted hazard ratios (95% CI) |
|---|---|---|
| 1–Most disadvantaged | 0.90 (0.67, 1.21) | 1.29 (0.96, 1.74) |
| 2 | 0.91 (0.67, 1.24) | 1.22 (0.90, 1.66) |
| 3 | 1.02 (0.74, 1.39) | 1.32 (0.97, 1.81) |
| 4 | 1.16 (0.82, 1.64) | 1.40 (1.01, 1.95) |
| 5–Least disadvantaged | Reference group | Reference group |
Residential remoteness
| Characteristic | Exposed to DFV adjusted hazard ratios b (95% CI) | No DFV exposure adjusted hazard ratios (95% CI) |
|---|---|---|
| Major cities | 1.37 (1.11, 1.68) | 1.19 (1.02, 1.39) |
| Inner regional | Reference group | Reference group |
| Outer regional | 1.14 (0.91, 1.42) | 1.00 (0.84, 1.18) |
| Remote | 1.16 (0.93, 1.45) | 1.01 (0.86, 1.20) |
| Very remote | 0.94 (0.77, 1.16) | 0.84 (0.72, 0.99) |
Maternal mental health contact a
| Characteristic | Exposed to DFV adjusted hazard ratios b (95% CI) | No DFV exposure adjusted hazard ratios (95% CI) |
|---|---|---|
| Yes | 0.87 (0.79, 0.95) | 1.10 (1.02, 1.20) |
| No | Reference group | Reference group |
Child has disability
| Characteristic | Exposed to DFV adjusted hazard ratios b (95% CI) | No DFV exposure adjusted hazard ratios (95% CI) |
|---|---|---|
| Yes | 1.28 (1.14 1.43) | 1.75 (1.59, 1.93) |
| No | Reference group | Reference group |
Notes: a Mother had a mental health diagnosis in HMDC or MHIS records that occurred prior to the child’s mental health episode.
b Multivariate analysis adjusted for all characteristic variables in table.
c Bold text denotes statistically significant estimates where the 95 per cent CIs did not include the null value.
Subcategories of mental health diagnosis
Aboriginal and Torres Strait Islander children
Following model adjustment, we observed that Aboriginal and Torres Strait Islander children exposed to DFV had a significantly higher risk of having a diagnosis in six of the 10 subcategories compared to their non-exposed peers (Figure 8), with significant risk increases ranging from 33 per cent for schizophrenia to 85 per cent for substance use. A 67 per cent increased risk of self-harm diagnosis was seen in Aboriginal and Torres Strait Islander children exposed to DFV compared with non-exposed Aboriginal and Torres Strait Islander children. Details of adjusted hazard ratios presented in Figure 8 can be found in Appendix D.
Figure 8: Risk of Aboriginal and Torres Strait Islander child with DFV exposure having a mental health subcategory compared to non-exposed Aboriginal and Torres Strait Islander children
| Mental health subcategory | Adjusted hazard ratios (95% CI) |
|---|---|
| Mental health contact with no diagnosis record | 1.45 (1.34, 1.57) |
| Other mental illness-related contacts | 1.07 (0.77, 1.51) |
| Intentional self-harm | 1.67 (1.31, 2.15) |
| Substance use disorder | 1.85 (1.52, 2.25) |
| Psychological development disorder | 1.10 (0.95, 1.27) |
| Depressive disorder | 1.30 (1.00, 1.70) |
| Anxiety disorder | 1.40 (1.25, 1.58) |
| Schizophrenia and psychoses | 1.33 (1.09, 1.61) |
| Personality disorder | 1.71 (0.96, 3.03) |
| Organic disorder | 1.68 (1.02, 2.76) |
Notes: Individual models were run for each subcategory. Models were adjusted for sex, early gestation (<37 weeks), mother’s age at birth, father’s age at birth, maternal marital status at birth, SES, residential remoteness, disability and maternal mental health contact. Risk estimates are presented as hazard ratios; error bars denote 95 per cent confidence intervals.
Non-Aboriginal and Torres Strait Islander children
Non-Aboriginal and Torres Strait Islander children exposed to DFV were observed to have a significantly higher risk of having a diagnosis in five of the 10 subcategories compared to their non-exposed peers, ranging from 22 per cent for psychological development to 148 per cent for substance use disorder (Figure 9). Details of adjusted hazard ratios presented in Figure 9 can be found in Appendix D.
Figure 9: Risk of non-Aboriginal and/or Torres Strait Islander child with DFV exposure having a mental health subcategory compared to non-exposed, non-Aboriginal and Torres Strait Islander children
| Mental health subcategory | Adjusted hazard ratios (95% CI) |
|---|---|
| Mental health contact with no diagnosis record | 1.56 (1.39, 1.75) |
| Other mental illness-related contacts | 1.35 (0.90, 2.03) |
| Intentional self-harm | 1.30 (0.90, 1.88) |
| Substance use disorder | 2.48 (1.52, 4.05) |
| Psychological development disorder | 1.22 (1.02, 1.45) |
| Depressive disorder | 1.36 (0.99, 1.87) |
| Anxiety disorder | 1.51 (1.31, 1.75) |
| Schizophrenia and psychoses | 1.42 (1.09, 1.86) |
| Personality disorder | 1.66 (0.95, 2.89) |
| Organic disorder | 0.99 (0.55, 1.77) |
Notes: Individual models were run for each subcategory. Models were adjusted for sex, early gestation (<37 weeks), mother’s age at birth, father’s age at birth, maternal marital status at birth, SES, residential remoteness, disability and maternal mental health contact. Risk estimates are presented as hazard ratios; error bars denote 95 per cent confidence intervals.
Disability
Characteristics associated with increased risk of mental health service contact in children with disability
Table 11 displays the characteristics associated with mental health service contact for both children with disability who are exposed to DFV and children with disability who are not exposed to DFV. Accounting for sociodemographic characteristics, children with disability exposed to DFV who were born pre-term (prior to 37 weeks gestation) were 23 per cent more likely to have a mental health service contact than DFV-exposed children born at term. Being born early was not associated with mental health service contact in children with disability not exposed to DFV.
For a child with disability and who was exposed to DFV, being born to a father aged over 40 years was associated with a 78 per cent increased risk of mental health service contact, compared with their DFV-exposed peers born to a father aged 30–39 years. However, father’s age was not associated with the risk of mental health service contact in children with disability but not exposed to DFV.
Maternal marital status at birth being unknown or missing in the Midwives Notification System was associated with a 116 per cent increase in the risk of mental health service contact in children with disability exposed to DFV compared to those DFV-exposed children with disability whose mother was married, widowed or in a de facto relationship. However, for children with disability who were not exposed to DFV the associated risk was 179 per cent. For children with disability who were not exposed to DFV, being born to a mother who was never married was associated with a 27 per cent increased risk of mental health service contact compared to non-exposed children with disability born to a mother who was married, widowed or in a de facto relationship. For children with disability who were exposed to DFV, being born to a mother who was never married had no observed relationship with risk of mental health service contact.
SES was not associated with the risk of mental health service contact in children with disability exposed to DFV. However, being from the most disadvantaged SES and from the second-most advantaged SES was associated with an increased risk of mental health service contact in children with disability not exposed to DFV (67% and 70% respectively).
Table 11: Risk of mental health service contact in childhood for children with disability and exposure to DFV and children with disability without exposure to DFV
Aboriginal and/or Torres Strait Islander
| Characteristic | Exposed to DFV adjusted hazard ratios b (95% CI) | No DFV exposure adjusted hazard ratios (95% CI) |
| Yes | 1.13 (0.92, 1.38) | 1.27 (1.08, 1.50) c |
| No | Reference group | Reference group |
Sex
| Characteristic | Exposed to DFV adjusted hazard ratios b (95% CI) | No DFV exposure adjusted hazard ratios (95% CI) |
|---|---|---|
| Female | 0.86 (0.73, 1.02) | 0.91 (0.80, 1.05) |
| Male | Reference group | Reference group |
Born prior to 37 weeks gestation
| Characteristic | Exposed to DFV adjusted hazard ratios b (95% CI) | No DFV exposure adjusted hazard ratios (95% CI) |
|---|---|---|
| Yes | 1.23 (1.02, 1.49) | 0.98 (0.82, 1.18) |
| No | Reference group | Reference group |
Mother’s age at birth
| Characteristic | Exposed to DFV adjusted hazard ratios b (95% CI) | No DFV exposure adjusted hazard ratios (95% CI) |
|---|---|---|
| <20 years | 0.78 (0.58, 1.05) | 1.22 (0.94, 1.58) |
| 20–29 years | 0.87 (0.69, 1.10) | 1.08 (0.90, 1.29) |
| 30–39 years | Reference group | Reference group |
| 40+ years | 0.96 (0.42, 2.21) | 1.57 (0.98, 2.51) |
Father’s age at birth
| Characteristic | Exposed to DFV adjusted hazard ratios b (95% CI) | No DFV exposure adjusted hazard ratios (95% CI) |
|---|---|---|
| <20 years | 1.21 (0.79, 1.85) | 0.86 (0.59, 1.26) |
| 20–29 years | 1.37 (1.05, 1.78) | 0.98 (0.82, 1.18) |
| 30–39 years | Reference group | Reference group |
| 40+ years | 1.78 (1.18, 2.69) | 1.08 (0.81, 1.43) |
| Missing age | 1.44 (1.08, 1.91) | 1.13 (0.89, 1.42) |
Maternal marital status at birth
| Characteristic | Exposed to DFV adjusted hazard ratios b (95% CI) | No DFV exposure adjusted hazard ratios (95% CI) |
|---|---|---|
| Married/de facto/widowed | Reference group | Reference group |
| Never married | 1.06 (0.88, 1.28) | 1.27 (1.06, 1.52) |
| Divorced/separated | 0.93 (0.53, 1.62) | 1.44 (0.89, 2.32) |
| Unknown/not stated | 2.16 (1.01, 4.59) | 2.79 (1.48, 5.26) |
Socioeconomic status
| Characteristic | Exposed to DFV adjusted hazard ratios b (95% CI) | No DFV exposure adjusted hazard ratios (95% CI) |
|---|---|---|
| 1–Most disadvantaged | 1.48 (0.91, 2.42) | 1.67 (1.04, 2.70) |
| 2 | 1.43 (0.86, 2.37) | 1.60 (0.98, 2.60) |
| 3 | 1.38 (0.82, 2.31) | 1.50 (0.91, 2.46) |
| 4 | 1.69 (0.97, 2.95) | 1.70 (1.02, 2.83) |
| 5–Least disadvantaged | Reference group | Reference group |
Residential remoteness
| Characteristic | Exposed to DFV adjusted hazard ratios b (95% CI) | No DFV exposure adjusted hazard ratios (95% CI) |
|---|---|---|
| Major cities | 1.39 (0.98, 1.96) | 0.90 (0.72, 1.13) |
| Inner regional | Reference group | Reference group |
| Outer regional | 1.18 (0.79, 1.76) | 0.95 (0.73, 1.24) |
| Remote | 1.11 (0.73, 1.70) | 0.85 (0.63, 1.13) |
| Very remote | 0.83 (0.56, 1.22) | 0.75 (0.56, 1.00) |
Maternal mental health contact a
| Characteristic | Exposed to DFV adjusted hazard ratios b (95% CI) | No DFV exposure adjusted hazard ratios (95% CI) |
|---|---|---|
| Yes | 0.96 (0.82, 1.14) | 1.16 (1.00, 1.35) |
| No | Reference group | Reference group |
Notes: a Mother had a mental health diagnosis in HMDC or MHIS records that occurred prior to the child’s mental health episode.
b Multivariate analysis adjusted for all characteristic variables in table.
c Bold text denotes statistically significant estimates where the 95 per cent CIs did not include the null value.
Subcategories of mental health diagnosis
In children with disability, exposure to DFV was associated with an increased risk of diagnosis in all mental health subcategories when compared to non-exposed children with disability (Figures 10 & 11). The level of risk increase ranged from 53 per cent for psychological development diagnosis to 74 per cent for personality disorder. Similarly, in children without disability, exposure to DFV was associated with an increased risk of diagnosis for all subcategories compared to non-exposed peers, ranging from 88 per cent for no diagnosis to 105 per cent increased risk in organic disorders and personality disorders. Further details of adjusted hazard ratios presented can be found in Appendix E.
Figure 10: Risk of children with disability exposed to DFV having a mental health subcategory compared to non-exposed children with disability
| Mental health subcategory | Adjusted hazard ratios (95% CI) |
|---|---|
| Mental health contact with no diagnosis record | 1.59 (1.44, 1.77) |
| Other mental illness-related contacts | 1.72 (1.55, 1.91) |
| Intentional self-harm | 1.73 (1.56, 1.92) |
| Substance use disorder | 1.72 (1.56, 1.91) |
| Psychological development disorder | 1.53 (1.38, 1.71) |
| Depressive disorder | 1.72 (1.55, 1.91) |
| Anxiety disorder | 1.63 (1.47, 1.81) |
| Schizophrenia and psychoses | 1.71 (1.54, 1.89) |
| Personality disorder | 1.74 (1.57, 1.93) |
| Organic disorder | 1.73 (1.57, 1.92) |
Notes: Individual models were run for each subcategory. Models were adjusted for sex, early gestation (<37 weeks), mother’s age at birth, father’s age at birth, maternal marital status at birth, SES, residential remoteness, disability and maternal mental health contact. Risk estimates are presented as hazard ratios; error bars denote 95 per cent confidence intervals.
Figure 11: Risk of children with no disability exposed to DFV having a mental health subcategory compared to non-exposed children with no disability
| Mental health subcategory | Adjusted hazard ratios (95% CI) |
|---|---|
| Mental health contact with no diagnosis record | 1.88 (1.78, 1.98) |
| Other mental illness-related contacts | 2.03 (1.93, 2.14) |
| Intentional self-harm | 2.02 (1.92, 2.13) |
| Substance use disorder | 2.02 (1.92, 2.13) |
| Psychological development disorder | 1.93 (1.83, 2.04) |
| Depressive disorder | 2.02 (1.91, 2.12) |
| Anxiety disorder | 1.92 (1.82, 2.03) |
| Schizophrenia and psychoses | 2.00 (1.90, 2.11) |
| Personality disorder | 2.05 (1.94, 2.16) |
| Organic disorder | 2.05 (1.94, 2.16) |
Notes: Individual models were run for each subcategory. Models were adjusted for sex, early gestation (<37 weeks), mother’s age at birth, father’s age at birth, maternal marital status at birth, SES, residential remoteness, disability and maternal mental health contact. Risk estimates are presented as hazard ratios; error bars denote 95 per cent confidence intervals.
Discussion
The aim of this research was to investigate the mental health service use of children exposed to DFV and the diagnosis subtypes of these children. We also aimed to identify sociodemographic characteristics that were predictive of diagnosis in children exposed to DFV. Additionally, we aimed to investigate the mental health service use and diagnosis of Aboriginal and Torres Strait Islander children and children with disability.
Mental health service contact
Findings from this research have shown that exposure to DFV in childhood is associated with an increased risk of mental health service contact during childhood. Our findings have some accord with existing research that acknowledges higher rates of DFV exposure in children using mental health services (Hultmann & Broberg, 2016; Ormhaug et al., 2012; Olaya et al., 2010). Hultmann and Broberg (2016) found that almost half of the children involved in Swedish mental health services had been exposed to DFV – five times higher than the rate of DFV in the general population. Our findings are different in that we measured mental health service contact in a DFV-exposed population and not DFV in a mental health service user population. Despite the differences, we have provided further robust evidence that DFV exposure is associated with an impact on children’s mental health.
The child’s involvement in mental health services should not necessarily be seen as a negative. Children exposed to DFV have experienced trauma and many are likely to need mental health services to aid them with addressing the trauma. However, it is concerning that, while the average age of exposure recorded in our data was 6.5 years, mental health service contact did not occur until the child was an average age of 12.5, similar to the service contact age in non-exposed children. Previous research has found that children exposed to trauma including DFV are more likely to need urgent mental health service access than those who have had no trauma exposure (Marshall et al., 2020). Early access to mental health services is important for children as it can reduce the long-term impact of mental illness (Colizzi et al., 2020; MacDonald et al., 2018). It is acknowledged that there are significant gaps in Australian mental health services for children aged0 to 12 (Australian Government, 2021), with psychiatric experts describing Australia’s mental health system as “broken” (National Mental Health Commission, 2020a). At present Australia’s mental health service is focused on specialist intervention not prevention and early intervention (Australian Government, 2021). However, the recently published National Children’s Mental Health and Wellbeing Strategy (Australian Government, 2021) aims to address these issues with priority given to children 0 to
12 years.
Early intervention is needed. This intervention should be underpinned by a public health approach addressing primary, secondary and tertiary prevention (Dahlberg & Krug, 2002; García-Moreno et al., 2015; Harvey et al., 2007). Investment is needed in primary prevention, that is, to prevent exposure before it occurs and hence eliminate subsequent negative outcomes. However, dual investment is needed in secondary and tertiary response and prevention measures to support the mental health of children exposed to DFV (National Mental Health Commission, 2020b). Early intervention for children’s mental health should address the impact of DFV exposure and its social determinants (Australian Government, 2021). This approach aligns with the National Children’s Mental Health and Wellbeing Strategy (Australian Government, 2021), which acknowledges the need to address the impact of trauma and socialdeterminants on children’s mental health and wellbeing. Without early intervention the child may potentially live with trauma and mental illness for many years impacting their ability to meet their full potential in education, relationships, employment and earning potential in adulthood (Altszuler et al., 2016; Australian Government, 2021; Clark et al., 2017; Colman et al., 2009; Erskine et al., 2016; McLeod & Kaiser, 2004). Additionally, it costs significantly more to treat mental illness in adolescence and adulthood than it does to intervene in early childhood (Teager et al., 2019). A further complexity is that the utilisation of health services for children exposed to DFV is multifaceted (Olaya et al., 2010; Onyskiw, 2002). Parents may not engage their child in mental health services for various reasons including fear of DFV being divulged by the child that may result in negative repercussions for mother and child from the perpetrator (Alaggia et al., 2011;Evans & Feder, 2016): mothers may be fearful of child removal if child protection services become involved (Alaggia et al., 2011; O’Donnell et al., 2015) and of the impact on the mother’s visa status if they are a dependant on their partner’s residency visa (Borges Jelinic, 2019). Additionally, there could be a delay due to the “sleeper effect” where symptoms may not manifest for many years after the exposure (Vu et al., 2016).
Diagnosis types
It is evident from our findings that exposure to DFV is associated with a significant impact on children’s mental health. This finding is in keeping with Bronfenbrenner’s (1977) theory that a child’s environment impacts human development. Children exposed to DFV were statistically more likely to have a higher risk in eight of the 10 mental health diagnosis subcategories than non-exposed children. The highest associated risk observed was a two-fold increased risk in substance use disorder. Our finding has some accord with previous longitudinal research that reported exposure to adverse childhood experiences, including DFV, was predictive of substance misuse (Rogers et al., 2021). Rogers and colleagues (2021) investigated substance misuse in children and young people from 14 to 26 years of age, finding that it increased at higher rates over time into early adulthood for children exposed to adverse events compared to those not exposed. The mental healthof our cohort was investigated until they reached 18 years of age. In light of the findings by Rogers and colleagues (2021) there is a need to investigate the mental health of children past childhood and into adulthood. For women subjected to DFV it is acknowledged that many misuse substances as a coping mechanism (Gezinski et al., 2021). For some children exposed to DFV substance use may also be a coping mechanism; further research is needed to gain a greater understanding of substance use in children exposed to DFV.
We also found an increased risk of personality disorder to be associated with DFV exposure. Personality disorders are thought to be caused by a combination of genetic and environmental factors, including trauma (Cattane et al., 2017). Our finding aligns with the cross-sectional research of Afifi and colleagues (2019) who found maltreatment in childhood, including DFV, was associated with an increased likelihood of personality disorder. Previous research has found a clear relationship between personality disorder and DFV perpetration and victimisation (Collison & Lynam, 2021; Jackson et al., 2015). Additionally, in some cases, children exposed to DFV may be at risk of becoming perpetrators or victims of DFV in adulthood (Ehrensaft et al., 2003; Smith et al., 2011). For the children exposed to DFV with personality disorder, it could be postulated that the risk of transgenerational abuse may be greater. The evidence, however, is not robust and, assuch, further research is clearly warranted to understand these complex associations more fully.
Exposure to DFV was associated with a 49 per cent increased risk of anxiety disorder, when compared to non-exposed children. While our findings align with recent Australian research (Gartland et al., 2021), some differences are noted. Gartland and colleagues (2021) reported a twofold increased likelihood of anxiety in children who were recently exposed to DFV which differs from our reported increase. The differences may be attributed to the approach used to identify anxiety and the differing ages between the studies. Gartland and colleagues measured anxiety at age 10, whereas the children’s anxiety in our cohort could be identified at any point in childhood. The key point, however, is that the children identified in our data as having their first mental health contact were, on average, aged 12.5 years, and therefore missing early childhood intervention. In consideration of Gartland’s findings and the Australian Government’s (2021) acknowledgement thatthere are service gaps in Australian mental health services for children aged 0 to 12 it is likely that our measurement of risk is an underestimation of the true association.
In keeping with existing literature (Huang et al., 2021; Kennedy et al., 2010; Kimball, 2016) we found that children’s exposure to DFV was associated with an increased risk of depression compared to non-exposed children. The aetiology of depression is multifactorial, with multiple ecological factors thought to play a part including genetics, exposure to stressful events (including DFV exposure) and low SES (Colman & Ataullahjan, 2010; Najman et al., 2010; Zalsman et al., 2006). As an example of the impact of low SES, recent international research (Marçal, 2021) has reported that housing insecurity mediates the risk of depression in children exposed to DFV. In Australia, utilising data from the Australian Specialist Homelessness Services Collection (AIHW, 2021c) would allow for the investigation of housing insecurity as a mediator of depression, and other outcomes, from an Australian perspective. A further advantage is that it would provide anotheravenue to identify DFV exposure as 42 per cent of clients seeking assistance from specialist homelessness services in Western Australia did so due to DFV (AIHW, 2019).
We found that, compared to non-exposed children, children exposed to DFV had a 52 per cent increased risk of having a mental health contact with no diagnosis recorded. This category captured children who were in MHIS data but had no diagnosis or had a mental health diagnosis in HMDC data or EDDC data. It is not clear from the data why this is the case; it may be for multiple reasons. The child may not engage in services to enable a diagnosis by clinicians. Additionally, the clinicians may be unaware of the DFV which prevents a full understanding of the child’s environment impacting clinical diagnosis. As discussed previously the lack of classification for developmental trauma may result in an absence of diagnosis so the child may not receive appropriate support and care. Further investigation is needed to gain an understanding of potential barriers in the support and treatment of children exposed to DFV.
The focus on diagnosis is highlighted in the National Children’s Mental Health and Wellbeing Strategy (Australian Government, 2021). The strategy proposes a cultural shift in the way that we think about the mental health and wellbeing of children – that is, a greater focus on a child’s functioning rather than diagnosis. The strategy argues that funded services should be available for children at the point that they begin to struggle, rather than delaying services until the child is unwell and is given a diagnosis. The strategy highlighted that this approach aligned with the Aboriginal and Torres Strait Islander concept of emotional wellbeing.
Predictive characteristics for mental health service contact
Overall, the characteristics that increased the risk of mental health service contact for children exposed to DFV were similar to those of non-exposed children. However, significant differences were noted in maternal age and mother’s mental health contact. For children exposed to DFV being born to a mother aged under 30 was associated with a reduced risk of mental health service contact. This reduction was not observed in the non-exposed children. Additionally, having a mother with a mental health service contact was associated with a 34 per cent increased risk of mental health service contact for non-exposed children, but it did not increase the risk for children exposed to DFV. It is not clear from our data why this is the case. Our findings are in contrast to existing literature that found parental mental illness can increase the risk of mental illness for the child (Matijasevich et al., 2014; Reupert et al., 2013). However, it is accepted that thecombination of DFV and maternal mental illness can disrupt parenting (Greene et al., 2018) which may reduce engagement in services for the child. Previous research has acknowledged the relationship between DFV and women’s mental health is complex and bidirectional in nature, with both highly associated with each other (Mason & O’Rinn, 2014). This may make the association of maternal mental illness and children’s mental illness harder to disentangle for families subjected to DFV. It should be noted that the reduction in risk for children exposed to DFV does not indicate that maternal mental illness or being born to a mother under 30 years are protective factors for mental health issues. Rather, these associations should be viewed as potential barriers that require further exploration.
Existing research is equivocal on whether sex impacts the mental health of children exposed to DFV (e.g. Sternberg et al., 2006). We found that, overall, sex had no impact on the risk of mental health service contact for children exposed to DFV. However, we did find differences in service use over time. Females exposed to DFV had lower probability of mental health service contact than their male counterparts between the age of 7 to 14. However, by the age of 15 years the probability of mental health service contact was similar for males and females. Our findings highlight the importance of investigating mental health service outcomes over an extended period. Without longitudinal research the association of characteristics on mental health for those exposed to DFV may be misinterpreted, impacting the ability to appropriately target services.
Differences in the sexes were noted in specific diagnosis subtypes. Being female increased the risk of personality disorder category in children exposed to DFV by 100 per cent and by 48 per cent in non-exposed children. Conversely, in the other mental illness-related contacts category higher risk was seen in non-exposed females who had a 291 per cent increased risk whereas exposed female children had a 100 per cent increased risk. Exposure to trauma in childhood is thought to increase the risk of personality disorder (Porter et al., 2020; Sher et al., 2015). The association of sex with personality disorders is complex, and findings from existing research are equivocal (Schulte Holthausen & Habel, 2018). One reason for the inconsistency is thought to be the influence of gender stereotypes on clinicians’ diagnosis of certain personality disorders (Crosby & Sprock, 2004; Schulte Holthausen & Habel, 2018). The higher risk of personalitydisorder seen in exposed females needs further investigation. It may be that there is greater bias in the diagnosis of personality disorder in females exposed to DFV due to gender stereotypes, or there may be some physiological underpinnings.
The findings on predictive characteristics support the proposal of ecological theory (Bronfenbrenner, 1977) that multiple variables influence a child’s mental health (D’Andrea & Graham-Bermann, 2017). Importantly, not all children with highlighted characteristics, such as a mother with mental illness or those who were born to a mother under 30 years, had a mental health contact or mental health diagnosis. This supports the theory (Bronfenbrenner & Morris, 2007) that developmental processes are probabilistic, not deterministic.
Aboriginal and Torres Strait
Islander children
Aboriginal and Torres Strait Islander children were overrepresented in our cohort with 62 per cent of children exposed to DFV being Aboriginal and Torres Strait Islander. This overrepresentation may be explained, in part, by high rates of DFV experienced by Aboriginal and Torres Strait Islander women, including mothers (ABS, 2016b; Orr, Preen et al., 2019). A further explanation for overrepresentation may be the source of our DFV identification: police and hospital data. Some studies suggest that the likelihood of being charged for DFV is increased by a variety of socioeconomic and demographic characteristics, such as Aboriginal status (Cunneen, 2010; Jeffries & Bond, 2015). Studies also show that Aboriginal and Torres Strait Islander women are more likely to be hospitalised for DFV than non-Aboriginal and Torres Strait Islander women (AIHW, 2006; Orr, Preen et al., 2019). DFV is not consistent with traditional Aboriginal and Torres Strait Islanderculture and the overrepresentation of Aboriginal and Torres Strait Islander children in this study should be understood in the context of the multiple disadvantages faced by Aboriginal and Torres Strait Islander peoples as a result of colonisation and not as an indicator of a racial determinant (Blagg et al., 2020; Our Watch, 2018). Additionally, Aboriginal and Torres Strait Islander women and children may be experiencing DFV perpetrated by non-Aboriginal and Torres Strait Islander people.
Similar to the full cohort, we found that for Aboriginal and Torres Strait Islander children who were exposed to DFV, having a mother with a mental health service contact reduced the risk of mental health service contact for the child. This was in contrast to the non-exposed children where an increase in service contact was noted. Findings from the Western Australian Aboriginal Child Health Survey (Zubrick et al., 2005) highlighted that Aboriginal children whose primary carer had used mental health services were more likely to have a mental health service use than those with a carer who had not used mental health services. However, the survey findings did not account for DFV exposure. Given the differences in mental health contact between children exposed to DFV and non-exposed children and the high rates of DFV in Aboriginal communities, future research investigating the mental health of Aboriginal and Torres StraitIslander children should consider the impact of
DFV exposure.
Our findings suggest that co-occurring DFV and maternal mental illness is a barrier to mental health service use for children exposed to DFV. A potential explanation may be that Aboriginal and Torres Strait Islander families experiencing multiple issues such as DFV and maternal and child mental illness are wary of service engagement due to fear of child removal (O’Donnell et al., 2015).
Both Aboriginal and Torres Strait Islander children exposed and not exposed to DFV had an increased risk of mental health service contact if they lived in a major city. This increase was not consistent with the full cohort where being from a major city had no impact on the risk of mental health service contact for both exposed and non-exposed children. Additionally, for Aboriginal and Torres Strait Islander children not exposed to DFV, living in a very remote location decreased their risk of mental health service contact by 16 per cent. However, for children exposed to DFV, being from a very remote area had no impact on the risk of mental health service contact. These findings cannot be taken to mean that children exposed to DFV out of the metropolitan area do not have as high a risk of mental illness – instead it may be due to the greater challenges in accessing mental health services outside the metropolitan area (National Mental Health Commission,2018). Previous research (Cassells et al., 2014) has reported that the lack of culturally appropriate mental health services for Aboriginal and Torres Strait Islander children living in remote and isolated communities is a barrier to accessing and engaging in services. Our findings have implications for regional and remote resource needs and mental health service provision to support children exposed to DFV. The newly launched Aboriginal Empowerment Strategy – Western Australia 2021–2029 (Government of Western Australia, 2021b) acknowledged the need for place-based partnership engagement. To ensure culturally responsive and secure services, services should be tailored to specific geographic areas to match local priorities and contexts, all while keeping Aboriginal culture at the forefront (Government of Western Australia, 2021b).
For Aboriginal and Torres Strait Islander children, exposure to DFV was associated with a significantly increased risk of intentional self-harm, which was not seen in non-exposed Aboriginal and Torres Strait Islander children but aligns with previous Australian research (Leckning et al., 2020). Self-harm is a major public health issue and is the leading cause of death in Australian children aged 5 to 17 (ABS, 2021b). The higher rates of intentional self-harm seen in Aboriginal and Torres Strait Islander children exposed to DFV have been attributed to the effects of intergenerational trauma stemming from the impacts of colonisation and Stolen Generation policies on family and community functioning (Dudgeon et al., 2017; Leckning et al., 2020). In addressing the high rates of intentional self-harm for Aboriginal and Torres Strait Islander children, the renewed Closing the Gap campaign (Commonwealth of Australia. Department of the Prime Minister andCabinet, 2021) recognises the need for strategies to promote high levels of social and emotional wellbeing. For some Aboriginal and Torres Strait Islander children and families, mainstream, western concepts of mental health do not directly translate into the more holistic framework of social and emotional wellbeing (Leckning et al., 2019). Aboriginal and Torres Strait Islander expertise in culturally appropriate service provision is needed to lead the way forward.
Our findings highlight the importance of Closing the Gap’s Target 13 – “families and households are safe” – which aims to reduce all forms of DFV against Aboriginal and Torres Strait Islander women and children by at least 50 per cent by 2031 (Commonwealth of Australia. Department of the Prime Minister and Cabinet 2021). Characteristics such as residential remoteness and maternal mental health contact were found to impact mental health service use and diagnosis in Aboriginal and Torres Strait Islander children, and these characteristics are worthy of further research. Aboriginal and Torres Strait Islander communities are best positioned to identify specific research questions to better understand the impact DFV exposure has on children’s mental health in their communities.
The Fourth National Action Plan of the National Plan to Reduce Violence against Women and their Children has prioritised support for Aboriginal women who are disproportionately exposed to DFV (Council of Australian Governments, 2019). There is a need for Aboriginal and Torres Strait Islander peoples to drive the development of multidisciplinary and multi-agency approaches that are both trauma informed and culturally appropriate for Aboriginal communities. To achieve this and to improve outcomes, government and service providers need to work in partnership with
Aboriginal communities.
Children with disability
To date, the impact of DFV on children with disability is poorly understood (Dababnah et al., 2018; Robinson et al., 2020). Our findings suggest that DFV exposure may be a barrier to service access for children with disability. For children exposed to DFV, having disability was associated with a 41 per cent increased chance of having a mental health service contact – that is, less than half the risk seen in non-exposed children with disability. Children with disability face multiple barriers accessing health services in a timely manner including cost, inadequate transportation, inaccessibility of buildings and discrimination by health professionals (AIHW, 2020b; VicHealth, 2012). For children exposed to DFV, the mother may not engage the child in mental health services for fear of child removal, since children with disability are more likely to have contact with child protection services and the out-of-home care system (Commonwealth of Australia, 2015;Hindmarsh et al., 2021). Further research is needed to gain a greater understanding of DFV exposure on mental health service access.
For children with disability who were exposed to DFV, being born pre-term (prior to 37 weeks gestation) was associated with an increased risk of mental health service contact. This increase was not observed in non-exposed peers. It is not clear from the data why pre-term birth is associated with an increased risk in children exposed to DFV. While our average age of exposure was 6.5 years, it is acknowledged that DFV can occur for many years before women report it or engage in services (Graham-Bermann & Perkins, 2010; Loxton et al., 2017). Therefore, it may be that some mothers were subjected to DFV while pregnant, which increases not only the risk of pre-term birth (Alhusen et al., 2015; Lipsky et al., 2003) but subsequent mental health issues for the child (Martinez-Torteya et al., 2015). Further research is required to gain a greater understanding of the association of pre-term birth and the mental health of children exposed to DFV, including thecapture of DFV in pregnancy.
Strengths and limitations
Strengths
The main strength of the research was the use of population level administrative data, linked across multiple agencies, at both the child and parent level to investigate the mental health of children exposed to DFV. The use of linked police and hospital data to identify DFV exposure enabled investigations of high-risk groups not captured in previous mental health research. Researching DFV is a complex task. The intimate context of the phenomenon means the act is not observed and, in many cases, is unreported (Phillips & Vandenbroek, 2014). The stigma related to the issue and the safety risk to the mothers and children also account for a high rate of non-responses within existing DFV research (Ruiz-Pérez et al., 2007). Identifying and researching children’s exposure to DFV is further complicated by maternal fear that their child may be removed if they disclose (Wilson et al., 2017). Due to these complexities, research related to childrenexposed to DFV is predominately based on small samples of children involved in specialist services, representing a subsection of those exposed. The use of the Western Australian Data Linkage System ensured that ethical and privacy standards were upheld and facilitated the ability to identify DFV and outcomes of a hidden population. The availability of dates of DFV events and outcome events allowed longitudinal follow-up. Additionally, the linked population data provided a wealth of information on multiple ecological factors at the child, parent and community level, enabling multivariate analysis when investigating the mental health of children exposed to DFV. The use of linked administrative data eliminated recall bias, reporting bias and loss-to-follow-up seen in existing literature.
As we had no information on the lived experiences of the children or families included in the study, our research was further strengthened by the community and consumer reference groups who aided interpretation of the findings.
Limitations
While the use of linked administrative data provides many advantages, there are some limitations that should be noted. While most violence against women is perpetrated by a current or former male intimate partner, it should be acknowledged that the DFV in some cases identified in the hospital data may have been perpetrated by someone other than a male intimate partner. DFV classification in hospital data is overly complex and needs to be streamlined to better capture the experiences of women.
Aboriginal and Torres Strait Islander children were overrepresented in our research cohort. This could be, in part, due to the police records of DFV requiring a charge to be made against the man; there is evidence to suggest that the likelihood of being charged for DFV is increased by a variety of socioeconomic and demographic characteristics, such as Aboriginal status (Australian Law Reform Commission, 2018; Cunneen, 2010; Jeffries & Bond, 2015). Despite a call-out occurring, on average, every 10 minutes in Western Australia for DFV, our exposed cohort comprised 5,736 mothers over five years. This equates to the number of call-outs police receive in 40 days. Therefore, our data are an underestimation of DFV and not generalisable to women who are victims of DFV where a man is not charged with an offence.
The children identified as exposed to DFV in this report were only recognised because of the mother’s involvement in police or hospital services. As such, the data may be subject to selection bias, capturing mainly the more physical cases of DFV, and may underestimate the impact of DFV exposure on children’s mental health outcomes due to the fact that not all children exposed to DFV were captured. It is therefore likely that the estimates presented in this report are conservative estimates of the association between DFV and the mental health of children exposed to DFV. Furthermore, it was assumed that the children exposed to DFV resided with their mother, but this may not be the case for all children captured.
Additionally, while rich data are made available from administrative datasets, the datasets provided no or limited data in relation to family functioning, family structure and social support. As such, there are likely to be a number of unmeasured characteristics that would have influenced outcomes for the child.
While the identification of disability was based on categories used in previous research (Maclean, Sims et al., 2017), the capture of disability is limited. Individuals differ on how they define their disability status and our definition does not take into account the complex and multidimensional nature of disability. Also, our definition is limited in its scope as it does not capture chronic health conditions such as asthma, epilepsy or permanent injuries which some of the literature incudes in its disability categories.
Our capture of mental illness in children was identified by public and private hospitalisations and ED attendance, and public outpatient mental health services. Many children with mental illness will not be identified in these data. The most recent Australian Child and Adolescent Survey of Mental Health and Wellbeing (Lawrence et al., 2015, p. 6) highlighted that only 6 per cent of children (4 to 17 years) with a mental health disorder had attended hospital or an emergency department for their mental health in the past 12 months. Furthermore, the survey highlighted that only 3 per cent of children (4 to 17 years) with mental illness had attended outpatient mental health services in the previous 12 months (Lawrence et al, 2015, p. 6). However, the survey found that 42 per cent of children had seen their GP for mental illness in the previous 12 months. Therefore, our identification of service use and diagnosis for childrenexposed to DFV is underestimated. Additionally, the findings of our results may not reflect those of children who have mental illness and use other services.
Distribution of categories within the cohort demographic characteristics varied. However, this was accounted for in the multivariable analysis employed from which the findings are reported. Finally, as an observational study, the results of the research contained in this report highlight an association, and do not indicate causality between DFV exposure and the development of mental illness.
Directions for future research
This report highlighted that there is a substantial period of time between children’s exposure to DFV and their contact with mental health services. Early access to mental health services is important for children as it can reduce the long-term impact of mental illness (MacDonald et al., 2018). It is imperative to ensure improved mental health outcomes for children exposed to DFV that research to understand factors associated with delay in service contact is undertaken as a priority. It is equally imperative that the results provide evidence to ensure the availability of adequate and appropriate services which can be accessed in a timely manner.
This report details the mental health service use and diagnosis of children exposed to DFV. It is acknowledged that children with mental health issues are more likely to have mental health issues in adulthood (Kessler, 2005; Ravens-Sieberer et al., 2015). Future research is needed to investigate the mental health of the children exposed to DFV into their adulthood. Additionally, further research is needed on the transition of care, for children exposed to DFV, from children’s mental health services to adult services. This transition period is often poorly managed (Crowley et al., 2011) with continuity of care disruption increasing disengagement from services (Singh, 2009). As young people with complex needs are at greater risk of “falling thorough the gaps” in care transition (Singh, 2009), attention to those exposed to DFV is needed.
Further research is required utilising multiple sources of linked data to identify both DFV and mental illness. Data sources such as the Australian Specialist Homelessness Services Collection (AIHW, 2021c), primary care general practice data, prescription data, school nurse data and private mental health outpatient services are required to gain a greater understanding of the effects of exposure to DFV on children’s mental health. The linked data should be complemented by combining data from population-based surveys, longitudinal surveys and social indicators (Hertzman & Williams, 2009). This multiple source approach would largely overcome the limitations of using each source separately and benefit from the strengths of each.
There is a need for research driven by Aboriginal and Torres Strait Islander peoples on the mental health of Aboriginal and Torres Strait Islander children given their disproportionate exposure to DFV. The findings contained in this report have the potential to be a stepping stone from which a holistic, culturally appropriate program of research can be developed.
We were unable to investigate the mental health service use of children born to CALD parents. Given that Australia continues to settle immigrants and those fleeing persecution and violence, having insufficient data available to undertake robust research to understand mental health outcomes and appropriate interventions in these populations is worrying. Ensuring that government and not-for-profit agencies routinely collect this data and make it available for research purposes is pivotal in enabling the urgently needed research.
Implications for policy and practice
Our research has shown that DFV exposure is associated with an increased risk of mental health service contact and diagnosis of mental illness. Early intervention is required. Many children exposed to DFV are not engaged in mental health services until years after the exposure. Our findings provide further support for the National Children’s Mental Health and Wellbeing Strategy (Australian Government, 2021) in that funded services should be available for children at the point that they begin to struggle, rather than services being delayed until the child is unwell and given a diagnosis. Our findings also add further support for the need for a dedicated standalone national response and matching actions strategy for the mental health of children exposed to DFV (Australian Government, 2021).
Children exposed to DFV often live with complex issues such as maternal mental illness and disability. Services to support children exposed to DFV must be well resourced and holistically focused with collaborative, multidisciplinary teams and cross-agency collaboration that provides continuity of care for children and their families with multiple and complex issues.
It is important that mental health clinicians are aware of trauma, including DFV exposure, during childhood. Clinicians need to have knowledge of DFV and its implications for mental health as well as the ability to appropriately and safely respond to children exposed to DFV (McTavish et al., 2016). These skills need to be taught to clinicians during their training and offered as ongoing professional development to enable clinicians to stay abreast of contemporary developments. At present DFV training is not part of the mandatory suite of training across Western Australian health services. A national approach should be taken to ensure that all registered and non-registered staff within public, private and NGO health services are provided with DFV training.
Aboriginal and Torres Strait Islander peoples should be provided with the opportunity and resources to develop policies and programs to support Aboriginal and Torres Strait Islander children who experience exposure to DFV.
Children and their families subjected to DFV are in contact with multiple agencies that may include education, health, police and child protection, and each agency provides a potential point of intervention. As such, it is imperative that these agencies, along with children’s mental health services, are embedded in, and part of, a broader collaborative, multiagency and multidisciplinary response to DFV; they need to be adapted to “fit” with the existing local response to DFV and to avoid unwarranted duplication of services.
To support service engagement and reduce the re-traumatisation of children exposed to DFV, service responses must be trauma informed and culturally responsive and secure.
Exposure to DFV is associated with an increased risk of mental health disorders in children. Our findings highlight the importance of the continuation of collective prevention efforts nationally and in each jurisdiction to reduce and eradicate DFV.
Conclusion
This study was undertaken to gain an understanding of the mental health service contact and diagnosis categories of children exposed to DFV. Using linked administrative data has enabled us to investigate a population that is often hidden. Children’s exposure to DFV is associated with an increased risk of mental health service use and mental health diagnosis in childhood. There are sociodemographic characteristics that appear to be factors associated with children exposed to DFV accessing mental health services including being born to a mother under 30 and a mother with mental illness. Additionally, many children are not accessing mental health services until several years after their exposure. These findings highlight the need for targeted government funding for early intervention mental health services for children exposed to DFV. Intervention strategies should be underpinned by a public health approach and include multidisciplinary, multi-agencyapproaches that are trauma-informed. Aboriginal and Torres Strait Islander children are overrepresented in our exposed cohort. This provides further evidence for the need to have culturally appropriate services led by and tailored for Aboriginal and Torres Strait Islander peoples.
References
Abel, K. M., Hope, H., Swift, E., Parisi, R., Ashcroft, D. M., Kosidou, K., Osam, C. S., Dalman, C., & Pierce, M. (2019). Prevalence of maternal mental illness among children and adolescents in the UK between 2005 and 2017: A national retrospective cohort analysis. Lancet Public Health, 4(6), e291–e300. https://doi.org/10.1016/S2468-2667(19)30059-3
Abrams, Z. (2021). Improved treatment for developmental trauma. American Psychological Association, 52(5), 38. https://www.apa.org/monitor/2021/07/ce-corner-developmental-trauma
Achenbach, T. (1991). Manual for the Child Behavior Checklist/4–18 and 1991 profile. University of Vermont Department of Psychiatry.
Afifi, T. O., Fortier, J., Sareen, J., & Taillieu, T. (2019). Associations of harsh physical punishment and child maltreatment in childhood with antisocial behaviors in adulthood. JAMA Network Open, 2(1), e187374. https://doi.org/10.1001/jamanetworkopen.2018.7374
Al-Yaman, F. (2017). The Australian Burden of Disease Study: Impact and causes of illness and death in Aboriginal and Torres Strait Islander people, 2011. Public Health Research & Practice, 27(4). https://doi.org/10.17061/phrp2741732
Alaggia, R., Regehr, C., & Jenney, A. (2012). Risky business: An ecological analysis of intimate partner violence disclosure. Research on Social Work Practice, 22(3), 301–312. https://doi.org/10.1177/1049731511425503
Alhusen, J. L., Ray, E., Sharps, P., & Bullock, L. (2015). Intimate partner violence during pregnancy: Maternal and neonatal outcomes. Journal of Women’s Health, 24(1), 100–106. https://doi.org/10.1089/jwh.2014.4872
Altszuler, A. R., Page, T. F., Gnagy, E. M., Coxe, S., Arrieta, A., Molina, B. S. G., & Pelham, W. E. (2016). Financial dependence of young adults with childhood ADHD. Journal of Abnormal Child Psychology, 44, 1217–1229. https://doi.org/10.1007/s10802-015-0093-9
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). American Psychiatric Association.
Anderson, D. M., Cesur, R., & Tekin, E. (2015). Youth depression and future criminal behavior. Economic Inquiry, 53(1), 294–317. https://doi.org/10.1111/ecin.12145
Antle, B., Barbee, A., Yankeelov, P., & Bledsoe, L. (2010). A qualitative evaluation of the effects of mandatory reporting of domestic violence on victims and their children. Journal of Family Social Work, 13, 56–73. https://doi.org/10.1080/10522150903468065
Australian Bureau of Statistics. (2011a). Australian and New Zealand Standard Offence Classification (ANZSOC), 2011. https://www.abs.gov.au/ausstats/[email protected]/mf/1234.0
Australian Bureau of Statistics. (2011b). 2006 Remoteness area from 2006 collection districts correspondence. https://www.abs.gov.au/ausstats/[email protected]/Products/1216.0.15.003~2006~Main+Features~2006+RA+from+2006+CD+Correspondence?OpenDocument
Australian Bureau of Statistics. (2016a). Disability, Ageing and Carers, Australia: Summary of findings, 2015 (ABS cat. no. 4430.0). https://www.abs.gov.au/ausstats/[email protected]/Lookup/4430.0main+features202015
Australian Bureau of Statistics. (2016b). National Aboriginal and Torres Strait Islander Social Survey 2014–15 (ABS cat. no. 4714.0). https://www.abs.gov.au/AUSSTATS/[email protected]/DetailsPage/4714.02014-15?OpenDocument
Australian Bureau of Statistics. (2017a). Personal Safety Survey 2016 (ABS cat. no. 4906.0). ABS.
Australian Bureau of Statistics. (2017b). 2016 Census QuickStats. https://quickstats.censusdata.abs.gov.au/census_services/getproduct/census/2016/quickstat/5?opendocument
Australian Bureau of Statistics. (2017c). Australian Demographic Statistics, December 2016. https://www.abs.gov.au/AUSSTATS/[email protected]/DetailsPage/3101.0Dec%202016?OpenDocument
Australian Bureau of Statistics. (2017d). Census of Population and Housing – Counts of Aboriginal and Torres Strait Islander Australians. https://www.abs.gov.au/statistics/people/aboriginal-and-torres-strait-islander-peoples/census-population-and-housing-counts-aboriginal-and-torres-strait-islander-australians/latest-release
Australian Bureau of Statistics. (2018a). Socio-economic indexes for areas. https://www.abs.gov.au/websitedbs/censushome.nsf/home/seifa
Australian Bureau of Statistics. (2018b). The Australian statistical geography standard (ASGS) remoteness structure. https://www.abs.gov.au/websitedbs/D3310114.nsf/home/remoteness+structure
Australian Bureau of Statistics. (2018c). Estimates of Aboriginal and Torres Strait Islander Australians. https://www.abs.gov.au/statistics/people/aboriginal-and-torres-strait-islander-peoples/estimates-aboriginal-and-torres-strait-islander-australians/latest-release#data-download
Australian Bureau of Statistics. (2019). Disability, Ageing and Carers, Australia: Summary of findings. https://www.abs.gov.au/statistics/health/disability/disability-ageing-and-carers-australia-summary-findings/latest-release#children-with-disability
Australian Bureau of Statistics. (2021a). 2016 Census QuickStats. https://quickstats.censusdata.abs.gov.au/census_services/getproduct/census/2016/quickstat/5?opendocument
Australian Bureau of Statistics. (2021b). Causes of death, Australia. https://www.abs.gov.au/statistics/health/causes-death/causes-death-australia/latest-release#intentional-self-harm-deaths-suicide-in-australia
Australian Early Development Census. (2022). About the AEDC data. https://www.aedc.gov.au/researchers/about-the-aedc-data
Australian Government. (2018). Data integration: Roles and responsibilities of data custodians. https://toolkit.data.gov.au/Data_Integration_-_Roles_and_responsibilities_of_data_custodians.html
Australian Government. (2021). National Children’s Mental Health and Wellbeing Strategy. https://www.mentalhealthcommission.gov.au/getmedia/e369a330-f8c3-4b9e-ab76-7a428f9ff0e3/national-childrens-mental-health-and-wellbeing-strategy-report-25oct2021
Australian Human Rights Commission. (2015). Face the facts: Aboriginal and Torres Strait Islander peoples. https://www.humanrights.gov.au/our-work/education/face-facts-aboriginal-and-torres-strait-islander-peoples
Australian Human Rights Commission. (2018). Information relating to Australia’s joint fifth and sixth report under the Convention on the Rights of the Child, second report on the Optional Protocol on the sale of children, child prostitution and child pornography, and second report on the Optional Protocol on the involvement of children in armed conflict. https://www.humanrights.gov.au/our-work/childrens-rights/publications/report-un-committee-rights-child-2018
Australian Institute of Family Studies. (2018). What is child abuse and neglect? https://aifs.gov.au/cfca/publications/what-child-abuse-and-neglect
Australian Institute of Health and Welfare. (2006). Family violence among Aboriginal and Torres Strait Islander peoples. https://www.aihw.gov.au/reports/indigenous-australians/family-violence-indigenous-peoples/contents/table-of-contents
Australian Institute of Health and Welfare. (2018a). Culturally and linguistically diverse populations. https://www.aihw.gov.au/getmedia/f3ba8e92-afb3-46d6-b64c-ebfc9c1f945d/aihw-aus-221-chapter-5-3.pdf.aspx
Australian Institute of Health and Welfare. (2018b). Family, domestic and sexual violence in Australia, 2018. https://www.aihw.gov.au/reports/domestic-violence/family-domestic-sexual-violence-in-australia-2018/contents/table-of-contents
Australian Institute of Health and Welfare. (2018c). Aboriginal and Torres Strait Islander adolescent and youth health and wellbeing 2018. https://www.aihw.gov.au/reports/indigenous-australians/atsi-adolescent-youth-health-wellbeing-2018/contents/summary
Australian Institute of Health and Welfare. (2019). Family, domestic and sexual violence in Australia: Continuing the national story. https://www.aihw.gov.au/getmedia/b0037b2d-a651-4abf-9f7b-00a85e3de528/aihw-fdv3-FDSV-in-Australia-2019.pdf.aspx?inline=true
Australian Institute of Health and Welfare. (2020a). Australia’s children: Chronic conditions and burden of disease. https://www.aihw.gov.au/reports/children-youth/australias-children/contents/health/chronic-conditions
Australian Institute of Health and Welfare. (2020b). People with disability in Australia. https://www.aihw.gov.au/reports/disability/people-with-disability-in-australia/contents/summary
Australian Institute of Health and Welfare. (2021a). Mental health services in Australia. https://www.aihw.gov.au/reports/mental-health-services/mental-health-services-in-australia/report-contents/expenditure-on-mental-health-related-services
Australian Institute of Health and Welfare. (2021b). Child protection Australia. https://www.aihw.gov.au/getmedia/c3b0e267-bd63-4b91-9ea6-9fa4d14c688c/aihw-cws-78.pdf.aspx?inline=true
Australian Institute of Health and Welfare. (2021c). Specialist Homelessness Services Collection. https://www.aihw.gov.au/about-our-data/our-data-collections/specialist-homelessness-services-collection
Australian Law Reform Commission. (2018). Pathways to justice: Inquiry into the incarceration rate of Aboriginal and Torres Strait Islander peoples (ALRC Report 133). https://www.alrc.gov.au/publication/pathways-to-justice-inquiry-into-the-incarceration-rate-of-aboriginal-and-torres-strait-islander-peoples-alrc-report-133/14-police-accountability/background-34/
Australia’s National Research Organisation for Women’s Safety. (2020a). Improving family violence legal and support services for Aboriginal and Torres Strait Islander peoples: Key findings and future directions (Research to policy and practice, 25–26/2020). ANROWS.
Australia’s National Research Organisation for Women’s Safety. (2020b). Australia’s National Research Agenda to Reduce Violence against Women and their Children: ANRA 2020–2022. ANROWS.
Bailey, B. A. (2010). Partner violence during pregnancy: Prevalence, effects, screening, and management. International Journal of Women’s Health, 2, 183–197. https://doi.org/10.2147/IJWH.S8632
Bair-Merritt, M., Johnson, S., Okelo, S., & Page, G. (2012). Intimate partner violence exposure, salivary cortisol, and childhood asthma. Child Abuse & Neglect, 36(7), 596–601. https://doi.org/10.1016/j.chiabu.2011.12.002
Bair-Merritt, M. H., Ghazarian, S. R., Burrell, L., Crowne, S. S., McFarlane, E., & Duggan, A. K. (2015). Understanding how intimate partner violence impacts school age children’s internalizing and externalizing problem behaviors: A secondary analysis of Hawaii Healthy Start Program evaluation data. Journal of Child & Adolescent Trauma, 8(4), 245–251. https://doi.org/10.1007/s40653-015-0066-8
Baldry, E., Bratel, J., & Breckenridge, J. (2006). Domestic violence and children with disabilities: Working towards enhancing social work practice. Australian Social Work, 59(2), 185–197. https://doi.org/10.1080/03124070600651895
Barker, E. D., Jaffee S. R., Uher, R., & Maughan, B. (2011). The contribution of prenatal and postnatal maternal anxiety and depression to child maladjustment. Depress Anxiety, 28, 696–702.
Bell, M. F., Bayliss, D. M., Glauert, R., & Ohan, J. L. (2018). Using linked data to investigate developmental vulnerabilities in children of convicted parents. Developmental Psychology, 54(7), 1219–1231. https://doi.org/10.1037/dev0000521
Berg, K., Bender, A., Evans, K., Holmes, M., Davis, A., Scaggs, A., & King, J. (2020). Service needs of children exposed to domestic violence: Qualitative findings from a statewide survey of domestic violence agencies. Children and Youth Services Review, 118, 105414. https://doi.org/10.1016/j.childyouth.2020.105414
Bidarra, Z. S., Lessard, G., & Dumont, A. (2016). Co-occurrence of intimate partner violence and child sexual abuse: Prevalence, risk factors and related issues. Child Abuse & Neglect, 55, 10–21. https://doi.org/10.1016/j.chiabu.2016.03.007
Blagg, H., Tulich, T., Hovane, V., Raye, D., Worrigal, T., & May, S. (2020). Understanding the role of Law and Culture in Aboriginal and/or Torres Strait Islander communities in responding to and preventing family violence, Ngarluma/Jaru/Gooniyandi (Hovane), Kimberley and Pilbara region, WA, Jabirr Jabirr/Bardi (Raye), Dampier Peninsula and Kimberley region, WA, Gooniyandi/Gija (Worrigal), Kimberley region, WA (Research report, 19/2020). ANROWS.
Boeckel, M. G., Wagner, A., & Grassi-Oliveira, R. (2017). The effects of intimate partner violence exposure on the maternal bond and PTSD symptoms of children. Journal of Interpersonal Violence, 32(7), 1127–1142. https://doi.org/10.1177/0886260515587667
Borges Jelinic, A. (2019). I loved him and he scared me: Migrant women, partner visas and domestic violence. Emotion, Space and Society, 32(May 2018), 100582. https://doi.org/10.1016/j.emospa.2019.100582
Bradley, A., & Dinan, T. (2010). A systematic review of hypothalamic-pituitary-adrenal axis function in schizophrenia: Implications for mortality. Journal of Psychopharmacology, 24(4), 91–118. https://doi.org/10.1177/1359786810385491
Bronfenbrenner, U. (1977). Towards an experimental ecology of human development. American Psychologist, 32(7), 513–531.
Bronfenbrenner, U. (1994). Ecological models of human development. In M. Gauvin & M. Cole (Eds.), Readings on the development of children (2nd ed.; pp. 37–43). Freeman.
Bronfenbrenner, U., & Morris, P. A. (2007). The bioecological model of human development. In R. M. Lerner & W. E. Damon (Eds.), Handbook of child psychology: Theoretical models of human development (pp. 793–828). Wiley.
Btoush, R., & Campbell, J. (2009). Ethical conduct in intimate partner violence research: Challenges and strategies. Nursing Outlook, 57(4), 210–216. https://doi:10.1016/j.outlook.2008.10.005
Buckley, H., Holt, S., & Whelan, S. (2007). Listen to me! Children’s experiences of domestic violence. Child Abuse Review, 16, 296–310. https://doi.org/10.1002/car.995
Calma, T., Dudgeon, P., & Bray, A. (2017). Aboriginal and Torres Strait Islander social and emotional wellbeing and mental health. Australian Psychologist, 52(4), 255–260. https://doi.org/10.1111/ap.12299
Campbell, K. A., Thomas, A. M., Cook, L. J., & Keenan, H. T. (2013). Resolution of intimate partner violence and child behavior problems after investigation for suspected child maltreatment. JAMA Pediatrics, 167(3), 236–242. https://doi.org/10.1001/2013.jamapediatrics.324
Campo, M. (2015). Children’s exposure to domestic and family violence: Key issues and responses. Australian Institute of Family Studies. https://aifs.gov.au/cfca/sites/default/files/publication-documents/cfca-36-children-exposure-fdv.pdf
Carline, A., & Easteal. P. (2014). Shades of grey: Domestic and sexual violence against women: Law reform and society. Routledge.
Carter, B., Paranjothy, S., Davies, A., & Kemp, A. (2020). Mediators and effect modifiers of the causal pathway between child exposure to domestic violence and internalizing behaviors among children and adolescents: A systematic literature review. Trauma, Violence, & Abuse. https://doi.org/10.1177/1524838020965964
Cassells, R., Cortis, N., Duncan, A., Eastman, C., Gao, G., Giuntoli, G., Katz, I., Keegan, M., Macvean, M., Mavisakalyan, A., Shlonsky, A., Skattebol, J., Smyth, C., & valentine, k. (2014). Keep them safe outcomes evaluation: Final report. Department of Premier and Cabinet. https://theirfuturesmatter.nsw.gov.au/__data/assets/pdf_file/0004/678946/KTS_Outcomes_Evaluation_Final_Report.pdf
Cattane, N., Rossi, R., Lanfredi, M., & Cattaneo, A. (2017). Borderline personality disorder and childhood trauma: Exploring the affected biological systems and mechanisms. BMC Psychiatry, 17(1), 221. https://doi.org/10.1186/s12888-017-1383-2
Chen, E., Turiano, N. A., Mroczek, D. K., & Miller, G. E. (2016). Association of reports of childhood abuse and all-cause mortality rates in women. JAMA Psychiatry, 73(9), 920–927. https://doi.org/10.1001/jamapsychiatry.2016.1786
Christensen, D., Davis, G., Draper, G., Mitrou, F., McKeown, S., Lawrence, D., McAullay, D., Pearson, G., Rikkers, W., & Zubrick, S. R. (2014). Evidence for the use of an algorithm in resolving inconsistent and missing Indigenous status in administrative data collections. Australian Journal of Social Issues, 49(4), 423–443. https://doi.org/10.1002/j.1839-4655.2014.tb00322.x
Cicchetti, D., & Valentino, K. (2006). An ecological transitional perspective on child maltreatment: Failure of the average expectable environment and its influence upon child development. In D. Cicchetti & D. J. Cohen, (Eds.), Developmental psychopathology (2nd ed.; pp. 129–201). Wiley.
Clark, A., Preen, D. B., Ng, J. Q., Semmens, J. B., & Holman, C. D. A. J. (2010). Is Western Australia representative of other Australian states and territories in terms of key socio-demographic and health economic indicators? Australian Health Review, 34(2), 210–215. https://doi.org/10.1071/AH09805
Clark, C., Smuk, M., Lain, D., Stansfeld, S. A., Carr, E., Head, J., & Vickerstaff, S. (2017). Impact of childhood and adulthood psychological health on labour force participation and exit in later life. Psychological Medicine, 47(9), 1597–1608. https://doi.org/10.1017/S0033291717000010
Cohen, S., Janicki-Deverts, D., & Miller, G. (2007). Psychological stress and disease. Journal of the American Medical Association, 298(14), 1685–1687. https://doi.org/10.1001/jama.298.14.1685
Colizzi, M., Lasalvia, A., & Ruggeri, M. (2020). Prevention and early intervention in youth mental health: Is it time for a multidisciplinary and trans-diagnostic model for care? International Journal of Mental Health Systems, 14(23). https://doi.org/10.1186/s13033-020-00356-9
Collins, J. (2013). Rethinking Australian immigration and immigrant settlement policy. Journal of Intercultural Studies, 34(2), 160–177. https://doi.org/10.1080/07256868.2013.781981
Collison, K. L., & Lynam, D. R. (2021). Personality disorders as predictors of intimate partner violence: A meta-analysis. Clinical Psychology Review, 88(August 2020), 102047. https://doi.org/10.1016/j.cpr.2021.102047
Colman, I., & Ataullahjan, A. (2010). Life course perspectives on the epidemiology of depression. Canadian Journal of Psychiatry, 55(10), 622–632. https://doi.org/10.1177/070674371005501002
Colman, I., Murray, J., Abbott, R. A., Maughan, B., Kuh, D., Croudace, T. J., & Jones, P. B. (2009). Outcomes of conduct problems in adolescence: 40-year follow-up of national cohort. BMJ (Online), 338(7688), 208–211. https://doi.org/10.1136/bmj.a2981
Commonwealth of Australia. (2015). Senate Standing Committees on Community Affairs: Out of home care report. https://www.aph.gov.au/Parliamentary_Business/Committees/Senate/Community_Affairs/Out_of_home_care/Report
Commonwealth of Australia. Department of the Prime Minister and Cabinet. (2021). National Agreement on Closing the Gap. Commonwealth of Australia.
Council of Australian Governments. (2011). National Plan to Reduce Violence against Women and their Children 2010–2022. https://www.dss.gov.au/women/programs-services/reducing-violence/the-national-plan-to-reduce-violence-against-women-and-their-children-2010-2022
Council of Australian Governments. (2015). National Outcome Standards for Perpetrator Interventions. https://plan4womenssafety.dss.gov.au/wp-content/uploads/2015/04/nospi_coag_paper.pdf
Council of Australian Governments. (2019). Fourth Action Plan of the National Plan to Reduce Violence against Women and their Children 2010–2022. https://www.dss.gov.au/women-publications-articles-reducing-violence/fourth-action-plan
Cox, P. (2015). Violence against women: Additional analysis of the Australian Bureau of Statistics’ Personal Safety Survey, 2012 (ANROWS Horizons, 01.01/2016, Rev. ed.). ANROWS.
Crosby, J. P., & Sprock, J. (2004). Effect of patient sex, clinician sex, and sex role on the diagnosis of antisocial personality disorder: Models of underpathologizing and overpathologizing biases. Journal of Clinical Psychology, 60(6), 583–604. https://doi.org/10.1002/jclp.10235
Crowley, R., Wolfe, I., Lock, K., & McKee, M. (2011). Improving the transition between paediatric and adult healthcare: A systematic review. Archives of Disease in Childhood, 96(6), 548–553. https://doi.org/10.1136/adc.2010.202473
Cunneen, C. (2010). Alternative and improved responses to domestic and family violence in Queensland Indigenous communities. University of New South Wales. https://documents.parliament.qld.gov.au/TableOffice/TabledPapers/2010/5310T1801.pdf
D’Andrea, W., & Graham-Berman, S. (2017). Social context and violence exposure as predictors of internalizing symptoms in mothers and children exposed to intimate partner violence. Journal of Family Violence, 32(2), 145–155. https://doi.org/10.1007/s10896-016-9869-0
Dababnah, S., Rizo, C. F., Campion, K., Downton, K. D., & Nichols, H. M. (2018). The relationship between children’s exposure to intimate partner violence and intellectual and developmental disabilities: A systematic review of the literature. American Journal on Intellectual and Developmental Disabilities, 123(6), 529–544. https://doi.org/10.1352/1944-7558-123.6.529
Dahlberg, L.L., & Krug, E.G. (2002). Violence – A global public health problem. In: E.G. Krug et al. (Eds.), World report on violence and health (pp. 3–21). World Health Organization.
Devaney, J. (2015). Research review: The impact of domestic violence on children. Irish Probation Journal, 12, 79–94.
Dobash, R. P., & Dobash, R. E. (1979). Violence against wives: A case against the patriarchy. Free Press.
Dudgeon, P., Calma, T., & Holland, C. (2017). The context and causes of the suicide of Indigenous people in Australia. Journal of Indigenous Wellbeing: Te Mauri, 2(2), 5–15. https://journalindigenouswellbeing.com/journal_articles/the-context-and-causes-of-the-suicide-of-indigenous-people-in-australia/
du Plessis, B., Kaminer, D., Hardy, A., & Benjamin, A. (2015). The contribution of different forms of violence exposure to internalizing and externalizing symptoms among young South African adolescents. Child Abuse & Neglect, 45, 80–89. https://doi.org/10.1016/j.chiabu.2015.02.021
Ehrensaft, M. K., Cohen, P., Brown, J., Smailes, E., Chen, H., & Johnson, J. G. (2003). Intergenerational transmission of partner violence: A 20-year prospective study. Journal of Consulting and Clinical Psychology, 71(4), 741–753. https://doi.org/10.1037/0022-006x.71.4.741
Ellsberg, M., & Heise, L. (2005) Researching violence against women: A practical guide for researchers and activists. World Health Organization.
Emerson, E., & Hatton, C. (2007). Mental health of children and adolescents with intellectual disabilities in Britain. British Journal of Psychiatry, 191(December), 493–499. https://doi.org/10.1192/bjp.bp.107.038729
Erskine, H. E., Norman, R. E., Ferrari, A. J., Chan, G. C. K., Copeland, W. E., Whiteford, H. A., & Scott, J. G. (2016). Long-term outcomes of attention-deficit/hyperactivity disorder and conduct disorder: A systematic review and meta-analysis. Journal of the American Academy of Child and Adolescent Psychiatry, 55(10), 841–850. https://doi.org/10.1016/j.jaac.2016.06.016
European Institute for Gender Inequality. (2017). Glossary of definitions of rape, femicide and intimate partner violence. https://eige.europa.eu/publications/glossary-definitions-rape-femicide-and-intimate-partner-violence
Evans, M. A., & Feder, G. S. (2016). Help-seeking amongst women survivors of domestic violence: A qualitative study of pathways towards formal and informal support. Health Expectations: An International Journal of Public Participation in Health Care and Health Policy, 19(1), 62–73. https://doi.org/10.1111/hex.12330
Evans, S. E., Davies, C., & Dilillo, D. (2008). Exposure to domestic violence: A meta-analysis of child and adolescent outcomes. Aggression and Violent Behavior, 13, 131–140.
Fantuzzo, J. W., & Lindquist, C. U. (1989). The effects of observing conjugal violence on children: A review and analysis of research methodology. Journal of Family Violence, 4(1), 77–94. https://doi.org/10.1007/BF00985658
Fergusson, D. M., Horwood, L. J., & Ridder, E. M. (2007). Conduct and attentional problems in childhood and adolescence and later substance use, abuse and dependence: Results of a 25-year longitudinal study. Drug and Alcohol Dependence, 88(Suppl.1), 14–26. https://doi.org/10.1016/j.drugalcdep.2006.12.011
Fisher, C. (2013). Changed and changing gender and family roles and domestic violence in African refugee background communities post-settlement in Perth, Australia. Violence Against Women, 19(7), 833–847. https://doi.org/10.1177/1077801213497535
Fisher, C., McKenzie, A., Preen, D., and Crowe, S., Cooke, V., Glauert, R., O’Donnell, M., Adams, I., West, M., Smith, S., Harrison, H., Nguyen, R., Henning, L., McNeil, N., & Frank, B. (2016). Family and domestic violence priority setting partnership project report. The University of Western Australia School of Population Health, Telethon Kids Institute, Kulunga Aboriginal Research Development Unit, Consumer and Community Health Research Network, Anglicare WA, Crowe Associates. https://www.anglicarewa.org.au/docs/default-source/who-we-are/research—family-and-communities/family-and-domestic-violence-priority-setting-partnership-project-report.pdf?sfvrsn=4d80ba5_2
Forns, M., Abad, J., & Kirchner T. (2018). Internalizing and externalizing problems. In R.J.R. Levesque (Ed.), Encyclopedia of adolescence. Springer. https://doi.org/10.1007/978-3-319-33228-4_261
Fraga, S. (2016). Methodological and ethical challenges in violence research. Porto Biomedical Journal, 1(2), 77–80. https://doi.org/10.1016/j.pbj.2016.04.005
Francis, L., Loxton, D., & James, C. (2017). The culture of pretence: A hidden barrier to recognising, disclosing and ending domestic violence. Journal of Clinical Nursing, 26(15–16), 2202–2214. https://doi.org/10.1111/jocn.13501
García-Moreno, C., Jansen, H.A., Ellsberg, M., Heise, L., & Watts, C. (2005). WHO multi-country study on women’s health and domestic violence against women: Initial results on prevalence, health outcomes and women’s responses. World Health Organization.
García-Moreno, C., Hegarty, K., d’Oliveira, A., Koziol-McLain, J., Colombini, M., & Feder, G. (2015). The health-systems response to violence against women. Lancet, 385(9977), 1567–1579. https://doi.org/10.1016/S0140-6736(14)61837-7
Gartland, D., Conway, L. J., Giallo, R., Mensah, F. K., Cook, F., Hegarty, K., Herrman, H., Nicholson, J., Reilly, S., Hiscock, H., Sciberras, E., & Brown, S. J. (2021). Intimate partner violence and child outcomes at age 10: A pregnancy cohort. Archives of Disease in Childhood, 1–9. https://doi.org/10.1136/archdischild-2020-320321
Gezinski, L. B., Gonzalez-Pons, K. M., & Rogers, M. M. (2021). Substance use as a coping mechanism for survivors of intimate partner violence: Implications for safety and service accessibility. Violence Against Women, 27(2), 108–123. https://doi.org/10.1177/1077801219882496
Ghafournia, N., & Easteal, P. (2018). Are immigrant women visible in Australian domestic violence reports that potentially influence policy? Laws, 7(4), 32. https://doi.org/10.3390/laws7040032
Gilbert, R., Widom, C. S., Browne, K., Fergusson, D., Webb, E., & Janson, S. (2009). Burden and consequences of child maltreatment in high-income countries. Lancet, 373(9657), 68–81.
Glasson, E. J., de Klerk, N. H., Bass, A. J. Rosman, D. L., Palmer, L. J., & Holman, C. D. J. (2008). Cohort profile: The Western Australian Family Connections Genealogical Project. International Journal of Epidemiology, 37(1), 30–35. https://doi.org/10.1093/ije/dym136
Goodsell, B., Lawrence, D., Ainley, J., Sawyer, M., Zubrick, S., & Maratos, J. (2017). Child and adolescent mental health and educational outcomes: An analysis of educational outcomes from Young Minds Matter: The second Australian Child and Adolescent Survey of Mental Health and Wellbeing. Young Minds Matter. https://youngmindsmatter.telethonkids.org.au/siteassets/media-docs—young-minds-matter/childandadolescent-mentalhealthandeducationaloutcomesdec2017.pdf
Government of Western Australia. (2015). Western Australian Family and Domestic Violence Common Risk Assessment and Risk Management Framework. https://www.wa.gov.au/government/document-collections/western-australian-family-and-domestic-violence-common-risk-assessment-and-risk-management-framework
Government of Western Australia. (2021b). Aboriginal Empowerment Strategy – Western Australia 2021–2029. https://www.wa.gov.au/organisation/department-of-the-premier-and-cabinet/aboriginal-empowerment-strategy-western-australia-2021-2029
Government of Western Australia Department of Health. (2022). Family connections. Data Linkage Western Australia. https://www.datalinkage-wa.org.au/dlb-services/family-connections/
Gracia, E., López-Quílez, A., Marco, M., & Lila, M. (2018). Neighborhood characteristics and violence behind closed doors: The spatial overlap of child maltreatment and intimate partner violence. PLOS One, 13(6), e0198684. https://doi.org/10.1371/journal.pone.0198684
Graham-Bermann, S. A. (2011). Child maltreatment in the context of intimate partner violence. In J. E. B. Myers (Ed.), The APSAC handbook on child maltreatment (3rd ed.; pp. 167–180). Sage.
Graham-Bermann, S. A., & Perkins, S. (2010). Effects of early exposure and lifetime exposure to intimate partner violence on child adjustment. Violence and Victims, 25(4), 427–439. https://doi.org/10.1891/0886-6708.25.4.427
Greene, C. A., Chan, G., McCarthy, K. J., Wakschlag, L. S., & Briggs-Gowan, M. J. (2018). Psychological and physical intimate partner violence and young children’s mental health: The role of maternal posttraumatic stress symptoms and parenting behaviors. Child Abuse & Neglect, 77, 168–179. https://doi.org/10.1016/j.chiabu.2018.01.012
Gray, R. J. (1988). A class of K-sample tests for comparing the cumulative incidence of a competing risk. Annals of Statistics,16, 1141–1154.
Hafekost, K., Lawrence, D., O’Leary, C., Bower, C., O’Donnell, M., Semmens, J., & Zubrick, S. R. (2017). Maternal alcohol use disorder and subsequent child protection contact: A record-linkage population cohort study. Child Abuse & Neglect, 72, 206–214. https://doi.org/10.1016/j.chiabu.2017.08.010
Hancock, K. J., Lawrence, D., Shepherd, C. C. J., Mitrou, F., & Zubrick, S. R. (2017). Associations between school absence and academic achievement: Do socioeconomics matter? British Educational Research Journal, 43(3), 415–440. https://doi.org/10.1002/berj.3267
Hansen, D., Lou, H.C., & Olsen, J. (2000). Serious life events and congenital malformations: A national study with complete follow-up. Lancet, 356(9233), 875–880.
Harron, K., Dibben, C., Boyd, J., Hjern, A., Azimaee, M., Barreto, M. L., & Goldstein, H. (2017). Challenges in administrative data linkage for research. Big Data & Society, 4(2). https://doi.org/10.1177/2053951717745678
Harvey, A., García-Moreno, C., & Butchart, A. (2007). Primary prevention of intimate partner violence and sexual violence: Background paper for WHO Expert Meeting May 2–3, 2007. World Health Organization. https://www.who.int/violence_injury_prevention/publications/violence/IPV-SV.pdf
Hebron, J., & Humphrey, N. (2014). Mental health difficulties among young people on the autistic spectrum in mainstream secondary schools: A comparative study. Journal of Research in Special Educational Needs, 14(1), 22–32. https://doi.org/10.1111/j.1471-3802.2012.01246.x
Heise, L. L. (1998). Violence against women: An integrated, ecological framework. Violence Against Women, 4(3), 262–290. https://doi.org/10.1177/1077801298004003002
Henderson, D. X., DeCuir-Gunby, J., & Gill, V. (2016). “It really takes a village”: A socio-ecological model of resilience for prevention among economically disadvantaged ethnic minority youth. Journal of Primary Prevention, 37, 469–485. https://doi.org/10.1007/s10935-016-0446-3
Herrman, H., Stewart, D. E., Diaz-Granados, N., Berger, E. L., Jackson, B., & Yuen, T. (2011). What is resilience? Canadian Journal of Psychiatry, 56(5), 258–265. https://doi.org/10.1177/070674371105600504
Herrenkohl, T. I., Sousa, C., Tajima, E. A., Herrenkohl, R. C., & Moylan, C. A. (2008). Intersection of child abuse and children’s exposure to domestic violence. Trauma, Violence & Abuse, 9, 84–99.
Hertzman, C., & Williams, R. (2009). Making early childhood count. Canadian Medical Association Journal, 180(1), 68–71. https://doi.org/10.1503/cmaj.080512
Heward-Belle, S., Humphreys, C., Healey, L., Toivonen, C., & Tsantefski, M. (2019). Invisible practices: Interventions with men who use violence and control. Affilia, 34(3), 369–382. https://doi.org/10.1177/0886109919848750
Hindmarsh, G., Laurens, K. R., Katz, I., Butler, M., Harris, F., Carr, V. J., & Green, M. J. (2021). Child protection services for children with special healthcare needs: A population record linkage study. Australian Journal of Social Issues, 56(2), 223–243. https://doi.org/10.1002/ajs4.145
Holden, G. W. (2003). Children exposed to domestic violence and child abuse: Terminology and taxonomy. Clinical Child and Family Psychology Review, 6, 151–160. https://doi.org/10.1023/A:1024906315255
Holman, C. D. J., Bass, A. J., Rosman, D. L., Smith, M. B., Semmens, J. B., Glasson, E. J., Brook, E. L., Trutwein, B., Rouse, I. L., Watson, C. R., de Klerk, N. H., Stanley, F. J., & Holman, C. J. (2008). A decade of data linkage in Western Australia: Strategic design, applications and benefits of the WA Data Linkage System. Australian Health Review, 32(4), 766–777. https://doi.org/10.1071/AH080766
Holman, C. D., Bass, A. J., Rouse, I. L., & Hobbs, M. S. (1999). Population-based linkage of health records in Western Australia: Development of a health services research linked database. Australian and New Zealand Journal of Public Health, 23(5), 453–459.
Holmes, M. R., Voith, L. A., & Gromoske, A. N. (2015). Lasting effect of intimate partner violence exposure during preschool on aggressive behavior and prosocial skills. Journal of Interpersonal Violence, 30(10), 1651–1670. https://doi.org/10.1177/0886260514552441
Hosokawa, R., & Katsura, T. (2019). Exposure to marital conflict: Gender differences in internalizing and externalizing problems among children. PLOS One, 14(9), 1–14. https://doi.org/10.1371/journal.pone.0222021
Howarth, E., Moore, T., Welton, N., Lewis, N., Stanley, N., MacMillan, H., Shaw, A., Hester, M., Bryden, P., & Feder, G. (2016). IMPRoving Outcomes for children exposed to domestic ViolencE (IMPROVE): An evidence synthesis. Public Health Research, 4(10), 1–342. https://doi.org/10.3310/phr04100
Howell, K. (2011). Resilience and psychopathology in children exposed to family violence. Aggression and Violent Behavior, 16(6), 562–569. https://doi.org/10.1016/j.avb.2011.09.001
Huang, C. C., Chen, Y., & Cheung, S. (2021). Early childhood exposure to intimate partner violence and teen depression symptoms in the U.S. Health and Social Care in the Community, 29(5), e47–e55. https://doi.org/10.1111/hsc.13240
Hultmann, O., & Broberg, A. G. (2016). Family violence and other potentially traumatic interpersonal events among 9- to 17-year-old children attending an outpatient psychiatric clinic. Journal of Interpersonal Violence, 31(18), 2958–2986. https://doi.org/10.1177/0886260515584335
Hultmann, O., Broberg, A. G., & Axberg, U. (2020). Child psychiatric patients exposed to intimate partner violence and/or abuse: The impact of double exposure. Journal of Interpersonal Violence 37(11–12), NP8611–NP8631. https://doi.org/10.1177/0886260520978186
Huth-Bocks, A. C., Levendosky, A. A., & Semel, M. A. (2001). The direct and indirect effects of domestic violence on young children’s intellectual functioning. Journal of Family Violence, 16, 269–290. https://doi.org/10.1023/A:1011138332712
Indermaur, D. (2001). Young Australians and domestic violence (Trends & Issues in Crime and Criminal Justice, no. 195). Australian Institute of Criminology. https://www.aic.gov.au/publications/tandi/tandi195
Izaguirre, A., & Calvete, E. (2018). Exposure to family violence and internalizing and externalizing problems among Spanish adolescents. Violence and Victims, 1(33), 368–382. https://doi.org/10.1891/0886-6708.VV-D-17-00016
Jackson, M. A., Sippel, L. M., Mota, N., Whalen, D., & Schumacher, J. A. (2015). Borderline personality disorder and related constructs as risk factors for intimate partner violence perpetration. Aggression and Violent Behavior, 24, 95–106. https://doi.org/10.1016/j.avb.2015.04.015
Jeffries, S., & Bond, C. E. (2015). Taking the problem seriously? Sentencing Indigenous and non-Indigenous domestic violence offenders. Australian & New Zealand Journal of Criminology, 48(4), 463–482. https://doi.org/10.1177/0004865814554306
Juruena, M. F., Eror, F., Cleare, A. J., & Young, A. H. (2020). The role of early life stress in HPA axis and anxiety. Advances in Experimental Medicine and Biology, 1191, 141–153. https://doi.org/10.1007/978-981-32-9705-0_9
Jutte, D. P., Roos, L., & Brownell, M.D. (2011). Administrative record linkage as a tool for public health research. Annual Review of Public Health, 32, 91–108.
Karakurt, G., Smith, D., & Whiting, J. (2014). Impact of intimate partner violence on women’s mental health. Journal of Family Violence, 29(7), 693–702.
Keeling, J., & Fisher, C. (2015). Health professionals’ responses to women’s disclosure of domestic violence. Journal of Interpersonal Violence, 30(13), 2363.
Kelman, C., Bass, A. J. & Holman, C. D. J. (2002). Research use of linked health data: A best practice protocol. Australian and New Zealand Journal of Public Health, 26(3), 251–255. https://doi.org/10.1111/j.1467-842X.2002.tb00682.x
Kennedy, A. C., Bybee, D., Sullivan, C. M., & Greeson, M. (2010). The impact of family and community violence on children’s depression trajectories: Examining the interactions of violence exposure, family social support, and gender. Journal of Family Psychology, 24(2), 197–207. https://doi.org/10.1037/a0018787
Kernic, M. A., Wolf, M. E., Holt, V. L., McKnight, B., Huebner, C. E., & Rivara, F. P. (2003). Behavioral problems among children whose mothers are abused by an intimate partner. Child Abuse & Neglect, 27(11), 1231–1246. https://doi.org/10.1016/j.chiabu.2002.12.001
Kessler, R. C., Berglund, P., Demler, O., Jin, R., Merikangas, K. R., & Walters, E. E. (2005). Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry, 62(6), 593–602. https://doi.org/10.1001/archpsyc.62.6.593
Kiecolt-Glaser, J., & Glaser, R. (2005). Stress-induced immune dysfunction: Implications for health. Nature Reviews Immunology, 5(3), 243–251. https://doi.org/10.1038/nri1571
Kimball, E. (2016). Edleson revisited: Reviewing children’s witnessing of domestic violence 15 years later. Journal of Family Violence, 31(5), 625–637. https://doi.org/10.1007/s10896-015-9786-7
Kitzmann, K. M., Gaylord, N. K., Holt, A. R., & Kenny, E. D. (2003). Child witnesses to domestic violence: A meta-analytic review. Journal of Consulting and Clinical Psychology, 71(2), 339–352. https://doi.org/10.1037/0022-006X.71.2.339
Kleinbaum, D. G., & Klein, M. (2012). Survival analysis: A self-learning text (3rd ed.). Springer.
Koenen, K., Moffitt, T., Caspi, A., Taylor, A., & Purcell, S. (2003). Domestic violence is associated with environmental suppression of IQ in young children. Development and Psychopathology, 15(2), 297–311. https://doi.org/10.1017/S0954579403000166
Korhonen, M., Luoma, I., Salmelin, R., & Tamminen, T. (2012). A longitudinal study of maternal prenatal, postnatal and concurrent depressive symptoms and adolescent well-being. Journal of Affective Disorders, 136, 680–692.
Leckning, B., Hirvonen, T., Armstrong, G., Carey, T. A., Westby, M., Ringbauer, A., & Robinson, G. (2020). Developing best practice guidelines for the psychosocial assessment of Aboriginal and Torres Strait Islander people presenting to hospital with self-harm and suicidal thoughts. Australian & New Zealand Journal of Psychiatry, 54(9), 874–882. https://doi.org/10.1177/0004867420924082
Leckning, B., Ringbauer, A., Robinson, G., Carey, T. A., Hirvonen, T., & Armstrong, G. (2019). Guidelines for best practice psychosocial assessment of Aboriginal and Torres Strait Islander people presenting to hospital with self-harm and suicidal thoughts. Menzies School of Health Research.
Lemerle, K., & Stewart, D. E. (2011). Resilience: Thriving beyond adversity. In S. Dillon & E. Mackinlay (Eds.), Meaningful music making for life series, book 3 (pp. 19–48). Cambridge Scholars Publishing.
Langdon, S., Armour, C., & Stringer, M. (2014). Adult experience of mental health outcomes as a result of intimate partner violence victimisation: A systematic review. European Journal of Psychotraumatology, 5(24794), 1–12. https://doi.org/10.3402/ejpt.v5.24794
Lawrence, D., Dawson, V., Houghton, S., Goodsell, B., & Sawyer, M. G. (2019). Impact of mental disorders on attendance at school. Australian Journal of Education, 63(1), 5–21. https://doi.org/10.1177/0004944118823576
Lawrence, D., Johnson, S., Hafekost, S., Boterhoven de Haan, K., Sawyer, M., Ainley, J., & Zubrick, S. (2015). The mental health of children and adolescents: Report on the Second Australian Child and Adolescent Survey of Mental Health and Wellbeing (Issue report). Department of Health.
Leis, J. A., Heron J, Stuart E. A., & Mendelson, T. (2014). Associations between maternal mental health and child emotional and behavioral problems: Does prenatal mental health matter? Journal of Abnormal Child Psychology, 42, 161–71.
Lipsky, S., Holt, V.L., Easterling, T.R., & Critchlow, C.W. (2003). Impact of police-reported intimate partner violence during pregnancy on birth outcomes. Obstetrics & Gynecology, 102(3), 557–564. https://doi.org/10.1016/S0029-7844(03)00573-8
Loxton, D., Townsend, N., Cavenagh, D., & Green, L. (2017). Measuring domestic violence in longitudinal research. Australian Government Department of Social Services. https://plan4womenssafety.dss.gov.au/wp-content/uploads/2018/07/Measuring-Domestic-Violence-in-Longitudinal-Research.pdf
Luthar, S. S., Cicchetti, D., & Becker, B. (2000). The construct of resilience: A critical evaluation and guidelines for future work. Child Development, 71(3), 543–562. https://doi.org/10.1111/1467-8624.00164
MacDonald, K., Fainman-Adelman, N., Anderson, K. K., & Iyer, S. N. (2018). Pathways to mental health services for young people: A systematic review. Social Psychiatry and Psychiatric Epidemiology, 53(10). https://doi.org/10.1007/s00127-018-1578-y
Maclean, M., Sims, S., Bower, C., Leonard, H., Stanley, F. J., & O’Donnell, M. (2017). Maltreatment risk among children with disabilities. Pediatrics, 139(4). https://doi.org/10.1542/peds.2016-1817
Maclean, M. J., Sims, S. A., & O’Donnell, M. (2019). Role of pre-existing adversity and child maltreatment on mental health outcomes for children involved in child protection: Population-based data linkage study. BMJ Open, 9(7), e029675. https://doi.org/10.1136/bmjopen-2019-029675
Maclean, M. J., Taylor, C. L., & O’Donnell, M. (2017). Relationship between out-of-home care placement history characteristics and educational achievement: A population level linked data study. Child Abuse & Neglect, 70(August 2017), 146–159. https://doi.org/10.1016/j.chiabu.2017.05.013
Maclean, M. J., Taylor, C. L., & O’Donnell, M. (2020). Adolescent education outcomes and maltreatment: The role of pre-existing adversity, level of child protection involvement, and school attendance. Child Abuse & Neglect, 109, 104721. https://doi.org/10.1016/j.chiabu.2020.104721
McGavock, L., & Spratt, T. (2017). Children exposed to domestic violence: Using adverse childhood experience scores to inform service response. British Journal of Social Work, 47(4), 1128–1146. https://doi.org/10.1093/bjsw/bcw073
McLeod, J. D., & Kaiser, K. (2004). Childhood emotional and behavioral problems and educational attainment. American Sociological Review, 9, 636–658.
McTavish, J. R., MacGregor, J. C. D., Wathen, C. N., & MacMillan, H. L. (2016). Children’s exposure to intimate partner violence: An overview. International Review of Psychiatry, 28(5), 504–518. https://doi.org/10.1080/09540261.2016.1205001
Marçal, K. E. (2021). Intimate partner violence exposure and adolescent mental health outcomes: The mediating role of housing insecurity. Journal of Interpersonal Violence, 1–21. https://doi.org/10.1177/08862605211043588
Margolin, G., & Gordis, E.B. (2000). The effects of family and community violence on children. Annual Review of Psychology, 51(1), 445–479.
Margolin, G., & Vickerman, K. (2007). Posttraumatic stress in children and adolescents exposed to family violence. Professional Psychology: Research and Practice, 38(6), 613–619. https://doi.org/10.1037/0735-7028.38.6.613
Marmot, M. (2011). Social determinants and the health of Indigenous Australians. Medical Journal of Australia, 194(10), 512–513.
Marshall, C., Semovski, V., & Stewart, S. L. (2020). Exposure to childhood interpersonal trauma and mental health service urgency. Child Abuse & Neglect, 106(March), 1–10. https://doi.org/10.1016/j.chiabu.2020.104464
Martinez-Torteya, C., Bogat, G. A., Levendosky, A. A., & Von Eye, A. (2015). The influence of prenatal intimate partner violence exposure on hypothalamic-pituitary-adrenal axis reactivity and childhood internalizing and externalizing symptoms. Development and Psychopathology, 28(1), 55–72. https://doi.org/10.1017/S0954579415000280
Mason, R., & O’Rinn, S. E. (2014). Co-occurring intimate partner violence, mental health, and substance use problems: A scoping review. Global Health Action, 7, 24815. https://doi.org/10.3402/gha.v7.24815
Masten, A. S. (2001) Ordinary magic: Resilience processes in development. American Psychologist, 56, 227–238.
Masten A. S. (2011). Resilience in children threatened by extreme adversity: Frameworks for research, practice, and translational synergy. Development and Psychopathology, 23(2), 493–506. https://doi.org/10.1017/S0954579411000198
Matijasevich, A., Murray, J., Cooper, P. J., Anselmi, L., Barros, A. J., Barros, F. C., & Santos, I. S. (2014). Trajectories of maternal depression and offspring psychopathology at 6 years: 2004 Pelotas cohort study. Journal of Affective Disorders, 174, 424–431. https://doi.org/10.1016/j.jad.2014.12.012
Mills, R., Scott, J., Alati, R., O’Callaghan, M., Najman, J. M., & Strathearn, L. (2012). Child maltreatment and adolescent mental health problems in a large birth cohort. Child Abuse & Neglect, 37(5), 292–302. https://doi.org/10.1016/j.chiabu.2012.11.008
Minas, H., Kakuma, R., Too, L. S., Vayani, H., Orapeleng, S., Prasad-Ildes, R., Turner, G., Procter, N., & Oehm, D. (2013). Mental health research and evaluation in multicultural Australia: Developing a culture of inclusion. Mental Health in Multicultural Australia (MHiMA), 7, Article 23. https://doi.org/10.1186/1752-4458-7-23
Moylan, C., Herrenkohl, T., Sousa, C., Tajima, E., Herrenkohl, R., & Russo, M. (2010). The effects of child abuse and exposure to domestic violence on adolescent internalizing and externalizing behavior problems. Journal of Family Violence, 25(1), 53–63. https://doi.org/10.1007/s10896-009-9269-9
Mueller, I., & Tronick, E. (2019). Early life exposure to violence: Developmental consequences on brain and behavior. Frontiers in Behavioral Neuroscience, 13, 156. https://doi.org/10.3389/fnbeh.2019.00156
Najman, J. M., Hayatbakhsh, M. R., Clavarino, A., Bor, W., O’Callaghan, M. J., & Williams, G. M. (2010). Family poverty over the early life course and recurrent adolescent and young adult anxiety and depression: A longitudinal study. American Journal of Public Health, 100(9), 1719–1723.
National Mental Health Commission. (2018). Australian Mental Health Commissions: Submission to the accessibility and quality of mental health services in rural and remote Australia Senate Inquiry [Submission]. https://www.nswmentalhealthcommission.com.au/sites/default/files/old/documents/mental_health_commissions_submission_-_mental_health_services_in_rural_and_remote_australia.pdf
National Mental Health Commission. (2020a). Children’s Mental Health and Wellbeing Strategy Consultations: January–February 2020. National Mental Health Commission.
National Mental Health Commission. (2020b). Inquiry into Family Domestic and Sexual Violence. https://www.mentalhealthcommission.gov.au/getmedia/f35003f4-5360-4f31-acee-efaa7c80c086/Submission-to-the-Inquiry-into-family-domestic-and-sexual-violence
National Scientific Council on the Developing Child. (2012). The science of neglect: The persistent absence of responsive care disrupts the developing brain. Center on the Developing Child: Harvard University.
Nock, M. K., Kazdin, A. E., Hiripi, E., & Kessler, R. C. (2007). Lifetime prevalence, correlates, and persistence of oppositional defiant disorder: Results from the National Comorbidity Survey Replication. Journal of Child Psychology and Psychiatry and Allied Disciplines, 48(7), 703–713. https://doi.org/10.1111/j.1469-7610.2007.01733.x
O’Donnell, M., Maclean, M. J., Sims, S., Morgan, V. A., Leonard, H., & Stanley, F. J. (2015). Maternal mental health and risk of child protection involvement: Mental health diagnoses associated with increased risk. Journal of Epidemiology and Community Health, 69(12), 1175–1183. https://doi.org/10.1136/jech-2014-205240
Olaya, B., Ezpeleta, L., de la Osa, N., Granero, R., & Doménech, J. M. (2010). Mental health needs of children exposed to intimate partner violence seeking help from mental health services. Children and Youth Services Review, 32(7), 1004–1011. https://doi.org/10.1016/j.childyouth.2010.03.028
Olofsson, N., Lindqvist, K., Gådin, K., Bråbäck, L., & Danielsson, I. (2011). Physical and psychological symptoms and learning difficulties in children of women exposed and non-exposed to violence: A population-based study. International Journal of Public Health, 56(1), 89–96. https://doi.org/10.1007/s00038-010-0165-0
Onyskiw, J. E. (2002). Health and use of health services of children exposed to violence in their families. Canadian Journal of Public Health, 93(6), 416–420. https://doi.org/10.1007/BF03405028
Ormhaug, S. M., Jensen, T. K., Hukkelberg, S. S., Holt, T., & Egeland, K. E. (2012). Children’s trauma, hidden or forgotten? An inquiry into the traumatic experiences of children and adolescents in child and adolescent mental health care. Tidsskrift for Norsk Psykologforening, 49, 234–240.
Orr, C., Fisher, C. M., Glauert, R., Preen, D. B., & O’Donnell, M. (2020). A demographic profile of mothers and their children who are victims of family and domestic violence: Using linked police and hospital admissions data. Journal of Interpersonal Violence, 37(1–2), NP500–NP525. https://doi.org/10.1177/0886260520916272
Orr, C., Fisher, C., Preen, D., Glauert, R., & O’Donnell, M. (2020). Exposure to family and domestic violence is associated with increased childhood hospitalisations. PLOS One, 15(8), e0237251. https://doi.org/10.1371/journal.pone.0237251
Orr, C., Fisher, C., Sims, S., Preen, D., Glauert, R., & O’Donnell, M. (2019). Hospitalisations for maternal assault are associated with increased risk of child protection involvement. Child Abuse & Neglect, 95. https://doi.org/10.1016/j.chiabu.2019.05.007
Orr, C., Kelty, E., Fisher, C., O’Donnell, M., Glauert, R., & Preen, D. (2022). The lasting impact of family and domestic violence on neonatal health outcomes. Manuscript submitted for publication.
Orr, C., O’Donnell, M., Fisher, C., Bell, M. Glauert, R., & Preen, D. (2021). School readiness of children exposed to family and domestic violence. Journal of Interpersonal Violence, 27(7), 713–732 https://doi.org/10.1177/08862605211050099
Orr, C., Preen., D., Fisher, C., Sims, S., & O’Donnell, M. (2019). Trends in hospital admissions for intimate partner violence in Australian mothers with children born from 1990 to 2009. Journal of Interpersonal Violence, 36(15–16), 6988–7017. https://doi.org/10.1177/0886260519832905
Ortega-García, J. A., Soldin, O. P., Sánchez-Sauco, M. F., Cánovas-Conesa, A., Gomaríz-Peñalver, V., Jaimes-Vega, D.C., Perales, J. E., Cárceles-Alvarez, A., Martínez-Ros, M. T., & Ruiz, D. (2013). Violence against women and gastroschisis: A case-control study. International Journal of Environmental Research and Public Health, 10(10), 5178–5190. https://doi.org/10.3390/ijerph10105178
Our Watch. (2018). Changing the picture: A national resource to support the prevention of violence against Aboriginal and Torres Strait Islander women and their children. https://apo.org.au/sites/default/files/resource-files/2018-07/apo-nid182621.pdf
Överlien, C., & Hydén, M. (2009). Children’s actions when experiencing domestic violence. Childhood, 16(4), 479–496. https://doi.org/10.1177/0907568209343757
Paavilainen, E., Lepistö, S., & Flinck, A. (2014). Ethical issues in family violence research in healthcare settings. Nursing Ethics, 21(1), 43–52. https://doi.org/10.1177/0969733013486794
Pearson, H. (2015). Massive study to follow 80,000 British babies cancelled. Nature, 526, 620–621.
Papendick, M., Bohner, G., & Windman, S. (2017). “Passive victim – strong survivor”? Perceived meaning of labels applied to women who were raped. PLOS One, 12(5), e0177550–e0177550. https://doi.org/10.1371/journal.pone.0177550
Pham, T. T. Le, Berecki-Gisolf, J., Clapperton, A., O’Brien, K. S., Liu, S., & Gibson, K. (2021). Definitions of culturally and linguistically diverse (CALD): A literature review of epidemiological research in Australia. International Journal of Environmental Research and Public Health, 18(2), 1–23. https://doi.org/10.3390/ijerph18020737
Phillips, J., & Vandenbroek, P. (2014). Domestic and family violence in Australia: An overview of the issues (Parliamentary Library Research Paper). Parliament of Australia. https://www.aph.gov.au/About_Parliament/Parliamentary_Departments/Parliamentary_Library/pubs/rp/rp1415/ViolenceAust
Porter, C., Palmier-Claus, J., Branitsky, A., Mensell, W., Harwick, H., & Varese, F. (2020). Childhood adversity and borderline personality disorder: A meta-analysis. Acta Psychiatrica Scandinavica, 141, 6–20.
Ravens-Sieberer, U., Otto, C., Kriston, L., Rothenberger, A., Döpfner, M., Herpertz-Dahlmann, B., Barkmann, C., Schön, G., Hölling, H., Schulte-Markwort, M., Klasen, F., & BELLA Study Group (2015). The longitudinal BELLA study: Design, methods and first results on the course of mental health problems. European Child & Adolescent Psychiatry, 24(6), 651–663. https://doi.org/10.1007/s00787-014-0638-4
Reef, J., Van Meurs, I., Verhulst, F.C., & Van Der Ende, J. (2010). Children’s problems predict adults’ DSM-IV disorders across 24 years. Journal of the American Academy of Child and Adolescent Psychiatry, 49(11), 1117–1124. https://doi.org/10.1016/j.jaac.2010.08.002
Reichel, D. (2017). Determinants of intimate partner violence in Europe: The role of socioeconomic status, inequality, and partner behavior. Journal of Interpersonal Violence, 32(12), 1853–1873. https://doi.org/10.1177/0886260517698951
Reif, K., & Jaffe, P. (2019). Remembering the forgotten victims: Child-related themes in domestic violence fatality reviews. Child Abuse & Neglect, 98(September). https://doi.org/10.1016/j.chiabu.2019.104223
Reupert, A. E., Maybery, D. J., & Kowalenko, N. M. (2012). Children whose parents have a mental illness: Prevalence, need and treatment. Medical Journal of Australia, 1(April), 7–9. https://doi.org/10.5694/mjao11.11200
Richard, L., Gauvin, L., & Raine, K. (2011). Ecological models revisited: Their uses and evolution in health promotion over two decades. Annual Review of Public Health, 32(1), 307–326. https://doi.org/10.1146/annurev-publhealth-031210-101141
Richards, K. (2011). Children’s exposure to domestic violence in Australia (Trends & Issues in Crime and Criminal Justice, no. 419). Australian Institute of Criminology. https://eprints.qut.edu.au/65037/1/kelly.pdf
Robinson, S., valentine, k., Newton, B. J., Smyth, C., & Parmenter, N. (2020). Violence prevention and early intervention for mothers and children with disability: Building promising practice (Research report, 16/2020). ANROWS.
Rogers, C. J., Forster, M., Grigsby, T. J., Albers, L., Morales, C., & Unger, J. B. (2021). The impact of childhood trauma on substance use trajectories from adolescence to adulthood: Findings from a longitudinal Hispanic cohort study. Child Abuse & Neglect, 120(July 2020), 105200. https://doi.org/10.1016/j.chiabu.2021.105200
Royal Australian and New Zealand College of Psychiatrists. (2016). Children of parents with mental illness. https://www.ranzcp.org/news-policy/policy-and-advocacy/position-statements/children-of-parents-with-mental-illness
Ruiz-Pérez, I., Plazaola-Castaño, J., & Vives-Cases, C. (2007). Methodological issues in the study of violence against women. Journal of Epidemiology and Community Health, 61(Suppl. 2), 26–31. https://doi.org/10.1136/jech.2007.059907
Schulte Holthausen, B., & Habel, U. (2018). Sex differences in personality disorders. Current Psychiatry Reports, 20(12), 107. https://doi.org/10.1007/s11920-018-0975-y
Secretariat of National Aboriginal and Islander Child Care. (2017). Strong families, safe kids: Family violence response and prevention for Aboriginal and Torres Strait Islander children and families. https://www.snaicc.org.au/wp-content/uploads/2017/09/Strong_Families_Safe_Kids-Sep_2017.pdf
Segal, L., Doidge, J., Armfield, J. M., Gnanamanickam, E. S., Preen, D. B., Brown, D. S., & Nguyen, H. (2021). Association of child maltreatment with risk of death during childhood in South Australia. JAMA Network Open, 4(6), e2113221. https://doi.org/10.1001/jamanetworkopen.2021.13221
Seng, J. S., Graham-Bermann, S. A., Clark, M. K., McCarthy, A. M., & Ronis D. L. (2005). Posttraumatic stress disorder and physical comorbidity among female children and adolescents: Results from service-use data. Pediatrics, 116, 767–776.
Shepherd, C.C.J., Li, J., Cooper, M.N., Hopkins, K.D., & Farrant, B.M. (2017). The impact of racial discrimination on the health of Australian Indigenous children aged 5–10 years: Analysis of national longitudinal data. International Journal for Equity in Health, 16(1), 1–12. https://doi.org/10.1186/s12939-017-0612-0
Sher, L., Siever, L. J., Goodman, M., McNamara, M., Hazlett, E. A., Koenigsberg, H. W., & New, A. S. (2015). Gender differences in the clinical characteristics and psychiatric comorbidity in patients with antisocial personality disorder. Psychiatry Research, 229(3), 685–689. https://doi.org/10.1016/j.psychres.2015.08.022
Singh, S. P. (2009). Transition of care from child to adult mental health services: The great divide. Current Opinion in Psychiatry, 22(4), 386–390. https://doi.org/10.1097/YCO.0b013e32832c9221
Smith, C. A., Ireland, T. O., Park, A., Elwyn, L., & Thornberry, T. P. (2011). Intergenerational continuities and discontinuities in intimate partner violence: A two-generational prospective study. Journal of Interpersonal Violence, 26(18), 3720–3752. https://doi.org/10.1177/0886260511403751
Smith, M. (2004). Parental mental health: Disruptions to parenting and outcomes for children. Child & Family Social Work, 9(1), 3–11. https://doi.org/10.1111/j.1365-2206.2004.00312.x
Spilsbury, J. C., Kahana, S., Drotar, D., Creeden, R., Flannery, D. J., & Friedman, S. (2008). Profiles of behavioral problems in children who witness domestic violence. Violence and Victims, 23(1), 3–17. https://doi.org/10.1891/0886-6708.23.1.3
Sternberg, K.J., Baradaran, L.P., Abbott, C.B., Lamb, M.E., & Guterman, E. (2006). Type of violence, age, and gender differences in the effects of family violence on children’s behavior problems: A mega-analysis. Developmental Review, 26(1), 89–112. https://doi.org/10.1016/j.dr.2005.12.001
Study of Environment on Aboriginal Resilience and Child Health Investigators. (2010). The Study of Environment on Aboriginal Resilience and Child Health (SEARCH): Study protocol. BMC Public Health, 10(1), 287–287. https://doi.org/10.1186/1471-2458-10-287
Swanston, J., Bowyer, L., & Vetere, A. (2014). Towards a richer understanding of school-age children’s experiences of domestic violence: The voices of children and their mothers. Clinical Child Psychology and Psychiatry, 19(2), 184–201. https://doi.org/10.1177/1359104513485082
Teager, W., Fox, S., & Stafford, N. (2019). How Australia can invest early and return more: A new look at the $15b cost and opportunity. Early Intervention Foundation, The Front Project & CoLab at the Telethon Kids Institute.
Udo, I. E., Sharps, P., Bronner, Y., & Hossain, M. B. (2016). Maternal intimate partner violence: Relationships with language and neurological development of infants and toddlers. Maternal and Child Health Journal, 20(7), 1424–1431. https://doi.org/10.1007/s10995-016-1940-1.
UNICEF. (2006). Behind closed doors: The impact of domestic violence on children. https://www.unicef.org/media/files/BehindClosedDoors.pdf
United Nations General Assembly. (1989). United Nations Convention on the Rights of the Child. https://humanrights. gov.au/our-work/childrens-rights/convention-rights-child
VicHealth. (2012). Disability and health inequalities in Australia. https://www.vichealth.vic.gov.au/media-and-resources/publications/disability-and-health-inequalities-in-australia
Vilariño, M., Amado, B. G., Vázquez, M. J., & Arce, R. (2018). Psychological harm in women victims of intimate partner violence: Epidemiology and quantification of injury in mental health markers. Psychosocial Intervention, 27(3), 145–152. https://doi.org/10.5093/pi2018a23
Vittinghoff, E., Glidden, D. V., Shiboski, S. C., & McCulloch, C. E. (2012). Regression methods in biostatistics: Linear, logistic, survival, and repeated measures models (2nd ed.). Springer.
von Elm, E., Altman, D. G., Egger, M., Pocock, S. J., Gøtzsche, P. C., & Vandenbroucke, J.P. (2008). STROBE Initiative: The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Journal of Clinical Epidemiology, 61(4), 344–349.
Vu, N. L., Jouriles, E. N., McDonald, R., & Rosenfield, D. (2016). Children’s exposure to intimate partner violence: A meta-analysis of longitudinal associations with child adjustment problems. Clinical Psychology Review, 46, 25–33. https://doi.org/10.1016/j.cpr.2016.04.003
Wadman, R., Botting, N., Durkin, K., & Conti-Ramsden, G. (2011). Changes in emotional health symptoms in adolescents with specific language impairment. International Journal of Language and Communication Disorders, 46(6), 641–656. https://doi.org/10.1111/j.1460-6984.2011.00033.x
Walter, M., Lovett, R., Maher, B., Williamson, B., Prehn, J., Bodkin-Andrews, G., & Lee, V. (2021). Indigenous data sovereignty in the era of big data and open data. Australian Journal of Social Issues, 56(2), 143–156. https://doi.org/10.1002/ajs4.141
Wilson, M., Jones, J., Butler, T., Simpson, P., Gilles, M., Baldry, E., Levy, M., & Sullivan, E. (2017). Violence in the lives of incarcerated Aboriginal mothers in Western Australia. Sage Open, 7(1). https://doi.org/10.1177/2158244016686814
World Health Organization. (2011a). World report on disability. https://www.who.int/disabilities/world_report/2011/report.pdf
World Health Organization. (2011b). ICD-10: International statistical classification of diseases and related health problems (10th rev.). WHO.
World Health Organization. (2014). Violence against women: Intimate partner and sexual violence against women (Fact sheet no. 239). WHO.
World Health Organization. (2018). Mental health: Strengthening our response. https://www.who.int/news-room/fact-sheets/detail/mental-health-strengthening-our-response
World Health Organization. (2020a). Violence against women and the girl child: Intimate partner violence. https://worlds-women-2020-data-undesa.hub.arcgis.com/apps/intimate-partner-violence/explore
World Health Organization. (2020b). The ecological framework. https://www.who.int/violenceprevention/approach/ecology/en/
World Health Organization. (2022). The VPA approach. https://www.who.int/groups/violence-prevention-alliance/approach
Ybarra, G. J., Wilkens, S. L., & Lieberman, A. F. (2007). The influence of domestic violence on preschooler behavior and functioning. Journal of Family Violence, 22(1), 33–42. https://doi.org/10.1007/s10896-006-9054-y
Yodanis, C. L. (2004). Gender inequality, violence against women, and fear: A cross-national test of the feminist theory of violence against women. Journal of Interpersonal Violence, 19, 655–675. https://doi.org/10.1177/0886260504263868
Zalsman, G., Oquendo, M. A., Greenhill, L., Goldberg, P. H., Kamali, M., Martin, A., & Mann, J. J. (2006). Neurobiology of depression in children and adolescents. Child and Adolescent Psychiatric Clinics of North America, 15(4), 843–868. https://doi.org/10.1016/j.chc.2006.05.010
Zubrick, S. R., Silburn, S. R., Lawrence, D. M., Mitrou, F. G., Dalby, R. B., Blair, E. M., Griffin, J., Milroy, H., De Maio, J. A., Cox, A., & Li, J. (2005). The Western Australian Aboriginal Child Health Survey (WAACHS). Curtin University of Technology, & Telethon Institute for Child Health Research. https://www.telethonkids.org.au/our-research/aboriginal-health/waachs/
Legislation
Children and Community Services Act 2004 (WA).
Family Law Act 1975 (Cth).
Restraining Orders Act 1997 (WA).
Appendix A:
Australian and New Zealand Standard Offence Classification codes used to categorise DFV
| Description | Classification code |
|---|---|
| Murder | 0111 |
| Attempted murder | 0121 |
| Assault and injury | 0211, 0212, 0213, 0299 |
| Sexual assault | 0311, 0312 |
| Threatening behaviour | 0532 |
| Misuse of weapons | 1122 |
Source: Australian Bureau of Statistics. (2011). Australian and New Zealand Standard Offence Classification (ANZSOC). https://www.abs.gov.au/ausstats/[email protected]/mf/1234.0
Appendix B:
The association of DFV exposure on the risk (adjusted hazard ratios) of childhood mental health diagnosis by subcategory
The tables below provide the adjusted hazard ratios and 95 per cent confidence intervals (CIs) for the risk associated with DFV exposure on specific mental health diagnosis groups (relating to Figure 2 in the report). Individual models were run for each group. Adjustments were made for Aboriginal and Torres Strait Islander status, sex, early gestation (<37 weeks), mother’s age at birth, father’s age at birth, maternal marital status at birth, SES, residential remoteness, disability and maternal mental health contact. Bolded text in tables denotes statistically significant estimates where the 95 per cent CIs did not include the null value.
Mental health contact with no diagnosis recorded
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 1.52 (1.42, 1.62) |
| No | Reference group |
Other mental illness-related contacts
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 1.21 (0.94, 1.56) |
| No | Reference group |
Intentional self-harm
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 1.59 (1.30, 1.96) |
| No | Reference group |
Substance use disorder
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 1.99 (1.66, 2.38) |
| No | Reference group |
Psychological development disorder
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 1.19 (1.06, 1.33) |
| No | Reference group |
Depressive disorder
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 1.36 (1.11, 1.66) |
| No | Reference group |
Anxiety disorder
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 1.49 (1.37, 1.63) |
| No | Reference group |
Schizophrenia and psychoses
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 1.39 (1.19, 1.63) |
| No | Reference group |
Personality disorder
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 1.76 (1.18, 2.61) |
| No | Reference group |
Organic disorder
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 1.41 (0.97, 2.04) |
| No | Reference group |
Appendix C:
The association of sociodemographic characteristics on the risk of childhood mental health diagnosis by subcategory in children exposed to DFV and not exposed to DFV
Anxiety disorder
Aboriginal and/or Torres Strait Islander
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Yes | 0.98 (0.84, 1.14) | 1.09 (0.96, 1.25) |
| No | Reference group | Reference group |
Sex
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
| Female | 1.36 (1.20, 1.55) c | 1.48 (1.33, 1.65) |
| Male | Reference group | Reference group |
Preterm
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| <37 weeks | 0.94 (0.77, 1.14) | 1.02 (0.85, 1.22) |
| >37 weeks | Reference group | Reference group |
Mother’s age at birth
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| <20 years | 0.77 (0.61, 0.98) | 0.99 (0.80, 1.24) |
| 20–29 years | 0.77 (0.63, 0.93) | 0.99 (0.85, 1.15) |
| 30–39 years | Reference group | Reference group |
| 40+ years | 1.79 (0.93, 3.42) | 1.42 (0.91, 2.21) |
Father’s age at birth
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
| <20 years | 1.08 (0.79, 1.48) | 1.25 (0.94, 1.67) |
| 20–29 years | 1.16 (0.96, 1.41) | 1.11 (0.95, 1.29) |
| 30–39 years | Reference group | Reference group |
| 40+ years | 0.99 (0.68, 1.45) | 1.25 (0.98, 1.59) |
| Missing age | 1.25 (1.00, 1.55) | 1.21 (0.99, 1.48) |
Maternal marital status at birth
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Never married | 1.06 (0.91, 1.23) | 1.30 (1.12, 1.50) |
| Divorced/separated | 1.02 (0.66, 1.56) | 1.63 (1.11, 2.39) |
| Unknown/not stated | 1.22 (0.54, 2.73) | 2.07 (1.10, 3.87) |
| Married/de facto/widowed | Reference group | Reference group |
Socioeconomic status
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| 1–Most disadvantaged | 0.78 (0.56, 1.07) | 1.14 (0.84, 1.55) |
| 2 | 0.82 (0.59, 1.14) | 1.06 (0.78, 1.46) |
| 3 | 0.86 (0.61, 1.21) | 1.02 (0.74, 1.42) |
| 4 | 0.80 (0.55, 1.17) | 0.92 (0.65, 1.32) |
| 5–Least disadvantaged | Reference group | Reference group |
Residential remoteness
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Major cities | 1.19 (0.94, 1.50) | 1.04 (0.87, 1.26) |
| Outer regional | 0.81 (0.61, 1.08) | 0.86 (0.69, 1.07) |
| Remote | 0.91 (0.68, 1.22) | 0.84 (0.66, 1.06) |
| Very remote | 0.78 (0.59, 1.04) | 0.79 (0.62, 1.00) |
| Inner regional | Reference group | Reference group |
Maternal mental health contact b
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Yes | 1.14 (1.00, 1.30) | 1.59 (1.42, 1.79) |
| No | Reference group | Reference group |
Child has disability
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Yes | 1.31 (1.11, 1.54) | 1.61 (1.39, 1.86) |
| No | Reference group | Reference group |
Notes: a Adjusted for characteristics listed in table.
b Mother had a mental health diagnosis in HMDC or MHIS records that occurred prior to the child’s mental health contact.
c Bold text denotes statistically significant estimates where the 95 per cent CIs did not include the null value.
Psychological development disorder
Aboriginal and or Torres Strait Islander
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Yes | 0.88 (0.72, 1.07) | 1.04 (0.90, 1.22) |
| No | Reference group | Reference group |
Sex
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Female | 0.77 (0.65, 0.91) c | 0.61 (0.54, 0.70) |
| Male | Reference group | Reference group |
Preterm
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| <37 weeks | 1.35 (1.08, 1.69) | 1.02 (0.84, 1.25) |
| >37 weeks | Reference group | Reference group |
Mother’s age at birth
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| <20 years | 0.83 (0.60, 1.14) | 1.21 (0.95, 1.55) |
| 20–29 years | 0.98 (0.75, 1.26) | 0.93 (0.78, 1.10) |
| 30–39 years | Reference group | Reference group |
| 40+ years | 1.43 (0.62, 3.30) | 1.94 (1.29, 2.93) |
Father’s age at birth
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| < 20 years | 1.17 (0.77, 1.79) | 0.93 (0.66, 1.31) |
| 20–29 years | 1.31 (1.01, 1.71) | 1.06 (0.89, 1.26) |
| 30–39 years | Reference group | Reference group |
| 40+ years | 1.45 (0.92, 2.28) | 1.15 (0.88, 1.50) |
| Missing age | 1.45 (1.08, 1.94) | 1.17 (0.93, 1.47) |
Maternal marital status at birth
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Never married | 1.04 (0.86, 1.27) | 1.18 (0.99, 1.40) |
| Divorced/separated | 0.76 (0.40, 1.42) | 1.89 (1.27, 2.82) |
| Unknown/not stated | 1.69 (0.75, 3.80) | 2.06 (1.06, 4.00) |
| Married/de facto/widowed | Reference group | Reference group |
Socioeconomic status
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| 1–Most disadvantaged | 0.87 (0.57, 1.33) | 1.64 (1.10, 2.46) |
| 2 | 0.87 (0.56, 1.34) | 1.57 (1.04, 2.36) |
| 3 | 0.83 (0.53, 1.31) | 1.34 (0.87, 2.04) |
| 4 | 0.82 (0.50, 1.36) | 1.33 (0.85, 2.08) |
| 5–Least disadvantaged | Reference group | Reference group |
Residential remoteness
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Major cities | 1.48 (1.06, 2.05) | 1.28 (1.02, 1.60) |
| Outer regional | 1.15 (0.78, 1.69) | 0.99 (0.76, 1.29) |
| Remote | 1.20 (0.80, 1.80) | 0.92 (0.69, 1.22) |
| Very remote | 0.75 (0.50, 1.12) | 0.95 (0.71, 1.27) |
| Inner regional | Reference group | Reference group |
Maternal mental health contact b
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Yes | 0.99 (0.84, 1.17) | 1.36 (1.18, 1.56) |
| No | Reference group | Reference group |
Child has disability
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Yes | 2.67 (2.23, 3.20) | 3.28 (2.86, 3.76) |
| No | Reference group | Reference group |
Notes: a Adjusted for characteristics listed in table.
b Mother had a mental health diagnosis in HMDC or MHIS records that occurred prior to the child’s mental health contact.
c Bold text denotes statistically significant estimates where the 95 per cent CIs did not include the null value.
Depressive disorder
Aboriginal and/or Torres Strait Islander
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Yes | 0.78 (0.55, 1.12) | 1.02 (0.77, 1.35) |
| No | Reference group | Reference group |
Sex
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Female | 2.83 (2.04, 3.94) c | 2.81 (2.16, 3.66) |
| Male | Reference group | Reference group |
Preterm
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| <37 weeks | 1.13 (0.73, 1.74) | 0.74 (0.46, 1.18) |
| >37 weeks | Reference group | Reference group |
Mother’s age at birth
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| <20 years | 1.19 (0.66, 2.13) | 1.06 (0.65, 1.71) |
| 20–29 years | 1.11 (0.68, 1.82) | 1.02 (0.73, 1.41) |
| 30–39 years | Reference group | Reference group |
| 40+ years | 1.18 (0.16, 8.87) | 1.75 (0.68, 4.47) |
Father’s age at birth
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| <20 years | 0.88 (0.43, 1.80) | 1.08 (0.54, 2.14) |
| 20–29 years | 0.99 (0.63, 1.56) | 1.29 (0.93, 1.79) |
| 30–39 years | Reference group | Reference group |
| 40+ years | 1.80 (0.84, 3.85) | 1.41 (0.83, 2.37) |
| Missing age | 1.06 (0.63, 1.78) | 1.31 (0.83, 2.06) |
Maternal marital status at birth
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Never married | 1.10 (0.78, 1.55) | 1.06 (0.76, 1.48) |
| Divorced/separated | 0.28 (0.04, 2.01) | 1.76 (0.77, 4.03) |
| Unknown/not stated | Count too small | 2.16 (0.53, 8.81) |
| Married/de facto/widowed | Reference group | Reference group |
Socioeconomic status
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| 1–Most disadvantaged | 1.05 (0.48, 2.32) | 1.72 (0.75, 3.96) |
| 2 | 1.09 (0.48, 2.44) | 1.86 (0.80, 4.31) |
| 3 | 0.83 (0.35, 1.98) | 1.61 (0.67, 3.84) |
| 4 | 0.62 (0.22, 1.71) | 1.82 (0.74, 4.45) |
| 5–Least disadvantaged | Reference group | Reference group |
Residential remoteness
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Major cities | 1.06 (0.63, 1.80) | 1.03 (0.68, 1.56) |
| Outer regional | 0.89 (0.47, 1.67) | 1.36 (0.87, 2.13) |
| Remote | 0.92 (0.47, 1.80) | 0.91 (0.54, 1.53) |
| Very remote | 0.79 (0.42, 1.50) | 0.62 (0.35, 1.09) |
| Inner regional | Reference group | Reference group |
Maternal mental health contact b
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Yes | 1.14 (0.84, 1.54) | 1.42 (1.09, 1.84) |
| No | Reference group | Reference group |
Child has disability
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Yes | 1.72 (1.20, 2.46) | 1.11 (0.77, 1.60) |
| No | Reference group | Reference group |
Notes: a Adjusted for characteristics listed in table.
b Mother had a mental health diagnosis in HMDC or MHIS records that occurred prior to the child’s mental health contact.
c Bold text denotes statistically significant estimates where the 95 per cent CIs did not include the null value.
Mental health contact with no diagnosis recorded
Aboriginal and/or Torres Strait Islander
| Characteristic | DFV exposure adjusted hazard ratiosa (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Yes | 1.08 (0.96, 1.22) | 1.27 (1.15, 1.40) c |
| No | Reference group | Reference group |
Sex
| Characteristic | DFV exposure adjusted hazard ratiosa (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Female | 0.84 (0.77, 0.92) | 0.83 (0.77, 0.90) |
| Male | Reference group | Reference group |
Preterm
| Characteristic | DFV exposure adjusted hazard ratiosa (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| <37 weeks | 1.19 (1.04, 1.36) | 1.16 (1.02, 1.31) |
| >37 weeks | Reference group | Reference group |
Mother’s age at birth
| Characteristic | DFV exposure adjusted hazard ratiosa (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| <20 years | 0.83 (0.69, 0.98) | 1.26 (1.08, 1.47) |
| 20–29 years | 0.79 (0.69, 0.92) | 1.05 (0.94, 1.17) |
| 30–39 years | Reference group | Reference group |
| 40+ years | 1.17 (0.65, 2.09) | 1.09 (0.76, 1.55) |
Father’s age at birth
| Characteristic | DFV exposure adjusted hazard ratiosa (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| <20 years | 1.08 (0.87, 1.36) | 1.05 (0.86, 1.29) |
| 20–29 years | 1.07 (0.92, 1.24) | 1.01 (0.91, 1.13) |
| 30–39 years | Reference group | Reference group |
| 40+ years | 1.19 (0.91, 1.54) | 1.32 (1.11, 1.56) |
| Missing age | 1.05 (0.89, 1.24) | 1.17 (1.01, 1.34) |
Maternal marital status at birth
| Characteristic | DFV exposure adjusted hazard ratiosa (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Never married | 1.02 (0.91, 1.14) | 1.14 (1.02, 1.26) |
| Divorced/separated | 1.36 (1.01, 1.83) | 1.51 (1.12, 2.03) |
| Unknown/not stated | 1.89 (1.20, 2.98) | 1.85 (1.17, 2.91) |
| Married/de facto/widowed | Reference group | Reference group |
Socioeconomic status
| Characteristic | DFV exposure adjusted hazard ratiosa (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| 1–Most disadvantaged | 1.04 (0.79, 1.38) | 1.77 (1.34, 2.35) |
| 2 | 1.01 (0.75, 1.35) | 1.77 (1.33, 2.36) |
| 3 | 1.27 (0.95, 1.70) | 1.74 (1.30, 2.34) |
| 4 | 1.10 (0.80, 1.52) | 1.73 (1.27, 2.35) |
| 5–Least disadvantaged | Reference group | Reference group |
Residential remoteness
| Characteristic | DFV exposure adjusted hazard ratiosa (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Major cities | 0.92 (0.77, 1.10) | 0.93 (0.81, 1.07) |
| Outer regional | 1.07 (0.88, 1.32) | 1.02 (0.87, 1.19) |
| Remote | 1.21 (0.98, 1.49) | 1.23 (1.05, 1.44) |
| Very remote | 0.99 (0.81, 1.21) | 0.94 (0.79, 1.11) |
| Inner regional | Reference group | Reference group |
Maternal mental health contact b
| Characteristic | DFV exposure adjusted hazard ratiosa (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Yes | 0.91 (0.82, 1.00) | 1.23 (1.13, 1.35) |
| No | Reference group | Reference group |
Child has disability
| Characteristic | DFV exposure adjusted hazard ratiosa (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Yes | 1.02 (0.89, 1.16) | 1.52 (1.37, 1.69) |
| No | Reference group | Reference group |
Notes: a Adjusted for characteristics listed in table.
b Mother had a mental health diagnosis in HMDC or MHIS records that occurred prior to the child’s mental health contact.
c Bold text denotes statistically significant estimates where the 95 per cent CIs did not include the null value.
Other mental illness-related contacts
Aboriginal and/or Torres Strait Islander
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Yes | 0.72 (0.45, 1.17) | 0.58 (0.32, 1.08) |
| No | Reference group | Reference group |
Sex
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Female | 2.00 (1.33, 3.00) c | 3.91 (2.11, 7.25) |
| Male | Reference group | Reference group |
Preterm
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| <37 weeks | 1.14 (0.66, 1.97) | 1.31 (0.59, 2.92) |
| >37 weeks | Reference group | Reference group |
Mother’s age at birth
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| <20 years | 0.98 (0.47, 2.04) | 0.18 (0.05, 0.65) |
| 20–29 years | 0.97 (0.53, 1.76) | 0.83 (0.43, 1.61) |
| 30–39 years | Reference group | Reference group |
| 40+ years | 1.56 (0.20, 12.03) | Count too small |
Father’s age at birth
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| <20 years | 0.30 (0.06, 1.38) | 2.82 (0.66, 11.93) |
| 20–29 years | 1.21 (0.66, 2.20) | 1.30 (0.65, 2.61) |
| 30–39 years | Reference group | Reference group |
| 40+ years | 1.99 (0.76, 5.17) | Count too small |
| Missing age | 1.55 (0.79, 3.04) | 2.28 (0.96, 5.45) |
Maternal marital status at birth
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Never married | 0.80 (0.50, 1.30) | 2.26 (1.18, 4.31) |
| Divorced/separated | Count too small | Count too small |
| Unknown/not stated | 3.61 (0.87, 14.94) | Count too small |
| Married/de facto/widowed | Reference group | Reference group |
Socioeconomic status
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| 1–Most disadvantaged | 1.44 (0.44, 4.75) | 0.93 (0.27, 3.19) |
| 2 | 1.36 (0.40, 4.62) | 0.94 (0.27, 3.30) |
| 3 | 0.96 (0.26, 3.53) | 0.64 (0.16, 2.59) |
| 4 | 1.87 (0.51, 6.82) | 0.70 (0.16, 3.13) |
| 5–Least disadvantaged | Reference group | Reference group |
Residential remoteness
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Major cities | 1.34 (0.60, 3.00) | 1.90 (0.67, 5.39) |
| Outer regional | 1.85 (0.77, 4.42) | 1.55 (0.48, 4.97) |
| Remote | 1.47 (0.57, 3.80) | 1.33 (0.37, 4.81) |
| Very remote | 1.04 (0.41, 2.63) | 0.63 (0.14, 2.95) |
| Inner regional | Reference group | Reference group |
Maternal mental health contact b
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Yes | 1.03 (0.69, 1.53) | 2.23 (1.30, 3.82) |
| No | Reference group | Reference group |
Child has disability
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Yes | 2.49 (1.62, 3.84) | 0.85 (0.36, 1.98) |
| No | Reference group | Reference group |
Notes: a Adjusted for characteristics listed in table.
b Mother had a mental health diagnosis in HMDC or MHIS records that occurred prior to the child’s mental health contact.
c Bold text denotes statistically significant estimates where the 95 per cent CIs did not include the null value.
Intentional self-harm
Aboriginal and/or Torres Strait Islander
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Yes | 1.36 (0.95, 1.96) | 1.17 (0.86, 1.60) |
| No | Reference group | Reference group |
Sex
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Female | 2.81 (2.05, 3.87) c | 3.20 (2.39, 4.28) |
| Male | Reference group | Reference group |
Preterm
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| <37 weeks | 0.84 (0.54, 1.32) | 0.81 (0.51, 1.30) |
| >37 weeks | Reference group | Reference group |
Mother’s age at birth
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| <20 years | 0.56 (0.33, 0.95) | 0.78 (0.48, 1.27) |
| 20–29 years | 0.68 (0.44, 1.06) | 0.77 (0.54, 1.08) |
| 30–39 years | Reference group | Reference group |
| 40+ years | 1.22 (0.16, 9.05) | 2.10 (0.74, 5.93) |
Father’s age at birth
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| <20 years | 1.78 (0.87, 3.62) | 1.09 (0.52, 2.29) |
| 20–29 years | 1.57 (0.95, 2.58) | 1.34 (0.94, 1.91) |
| 30–39 years | Reference group | Reference group |
| 40+ years | 1.43 (0.58, 3.56) | 0.61 (0.29, 1.29) |
| Missing age | 1.89 (1.12, 3.22) | 1.71 (1.09, 2.69) |
Maternal marital status at birth
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Never married | 1.29 (0.93, 1.78) | 1.10 (0.78, 1.56) |
| Divorced/separated | 0.77 (0.24, 2.45) | 0.91 (0.29, 2.90) |
| Unknown/not stated | Count too small | 1.09 (0.15, 7.84) |
| Married/de facto/widowed | Reference group | Reference group |
Socioeconomic status
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| 1–Most disadvantaged | 1.53 (0.55, 4.22) | 1.03 (0.49, 2.16) |
| 2 | 1.62 (0.58, 4.58) | 1.08 (0.51, 2.28) |
| 3 | 2.00 (0.70, 5.71) | 0.86 (0.39, 1.92) |
| 4 | 1.18 (0.36, 3.85) | 0.98 (0.43, 2.27) |
| 5–Least disadvantaged | Reference group | Reference group |
Residential remoteness
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Major cities | 0.85 (0.52, 1.40) | 0.76 (0.50, 1.16) |
| Outer regional | 0.48 (0.25, 0.93) | 0.96 (0.60, 1.53) |
| Remote | 0.79 (0.43, 1.44) | 0.67 (0.39, 1.14) |
| Very remote | 0.62 (0.35, 1.11) | 0.78 (0.47, 1.30) |
| Inner regional | Reference group | Reference group |
Maternal mental health contact b
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Yes | 1.07 (0.80, 1.44) | 1.42 (1.07, 1.87) |
| No | Reference group | Reference group |
Child has disability
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Yes | 1.55 (1.09, 2.21) | 1.03 (0.69, 1.54) |
| No | Reference group | Reference group |
Notes: a Adjusted for characteristics listed in table.
b Mother had a mental health diagnosis in HMDC or MHIS records that occurred prior to the child’s mental health contact.
c Bold text denotes statistically significant estimates where the 95 per cent CIs did not include the null value.
Substance use disorder
Aboriginal and/or Torres Strait Islander
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Yes | 2.92 (2.05, 4.16) c | 4.59 (3.13, 6.75) |
| No | Reference group | Reference group |
Sex
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Female | 1.10 (0.86, 1.40) | 0.83 (0.64, 1.06) |
| Male | Reference group | Reference group |
Preterm
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| <37 weeks | 1.14 (0.82, 1.59) | 1.21 (0.84, 1.74) |
| >37 weeks | Reference group | Reference group |
Mother’s age at birth
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| <20 years | 1.29 (0.81, 2.05) | 0.95 (0.60, 1.50) |
| 20–29 years | 1.04 (0.69, 1.57) | 0.89 (0.62, 1.27) |
| 30–39 years | Reference group | Reference group |
| 40+ years | 1.00 (0.14, 7.38) | 0.97 (0.23, 4.10) |
Father’s age at birth
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| <20 years | 0.89 (0.51, 1.57) | 0.87 (0.44, 1.70) |
| 20–29 years | 0.76 (0.51, 1.15) | 1.11 (0.76, 1.61) |
| 30–39 years | Reference group | Reference group |
| 40+ years | 1.29 (0.62, 2.70) | 1.10 (0.55, 2.20) |
| Missing age | 1.37 (0.91, 2.08) | 1.79 (1.18, 2.71) |
Maternal marital status at birth
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Never married | 0.99 (0.75, 1.30) | 1.22 (0.90, 1.65) |
| Divorced/separated | 0.75 (0.27, 2.03) | 0.78 (0.25, 2.47) |
| Unknown/not stated | 0.83 (0.12, 5.94) | 3.63 (1.33, 9.89) |
| Married/de facto/widowed | Reference group | Reference group |
Socioeconomic status
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| 1–Most disadvantaged | 1.08 (0.52, 2.23) | 0.80 (0.40, 1.59) |
| 2 | 0.78 (0.36, 1.67) | 0.43 (0.20, 0.91) |
| 3 | 0.83 (0.38, 1.84) | 0.52 (0.24, 1.14) |
| 4 | 1.11 (0.47, 2.60) | 0.91 (0.41, 2.00) |
| 5–Least disadvantaged | Reference group | Reference group |
Residential remoteness
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Major cities | 1.17 (0.73, 1.87) | 0.94 (0.60, 1.45) |
| Outer regional | 0.78 (0.45, 1.35) | 0.73 (0.44, 1.20) |
| Remote | 0.78 (0.45, 1.36) | 0.58 (0.34, 0.99) |
| Very remote | 0.59 (0.35, 0.99) | 0.64 (0.39, 1.06) |
| Inner regional | Reference group | Reference group |
Maternal mental health contact b
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Yes | 0.86 (0.67, 1.10) | 1.28 (0.98, 1.67) |
| No | Reference group | Reference group |
Child has disability
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Yes | 1.80 (1.37, 2.38) | 1.75 (1.28, 2.38) |
| No | Reference group | Reference group |
Notes: a Adjusted for characteristics listed in table.
b Mother had a mental health diagnosis in HMDC or MHIS records that occurred prior to the child’s mental health contact.
c Bold text denotes statistically significant estimates where the 95 per cent CIs did not include the null value.
Schizophrenia and psychoses
Aboriginal and/or Torres Strait Islander
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Yes | 0.98 (0.74, 1.29) | 1.26 (1.00, 1.57) |
| No | Reference group | Reference group |
Sex
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Female | 1.95 (1.54, 2.48) c | 2.08 (1.72, 2.53) |
| Male | Reference group | Reference group |
Preterm
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| <37 weeks | 0.98 (0.69, 1.39) | 0.59 (0.40, 0.87) |
| >37 weeks | Reference group | Reference group |
Mother’s age at birth
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| <20 years | 1.51 (0.94, 2.41) | 0.94 (0.65, 1.36) |
| 20–29 years | 1.34 (0.89, 2.02) | 0.95 (0.73, 1.22) |
| 30–39 years | Reference group | Reference group |
| 40+ years | 1.88 (0.44, 7.94) | 1.51 (0.69, 3.30) |
Father’s age at birth
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| <20 years | 0.98 (0.57, 1.67) | 1.08 (0.64, 1.81) |
| 20–29 years | 0.98 (0.69, 1.41) | 1.12 (0.87, 1.45) |
| 30–39 years | Reference group | Reference group |
| 40+ years | 1.64 (0.86, 3.14) | 1.23 (0.80, 1.87) |
| Missing age | 1.22 (0.81, 1.82) | 1.41 (1.01, 1.98) |
Maternal marital status at birth
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Never married | 1.06 (0.82, 1.38) | 1.08 (0.83, 1.39) |
| Divorced/separated | 0.53 (0.17, 1.67) | 1.50 (0.77, 2.95) |
| Unknown/not stated | 1.63 (0.40, 6.60) | 2.58 (0.95, 6.98) |
| Married/de facto/widowed | Reference group | Reference group |
Socioeconomic status
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| 1–Most disadvantaged | 1.06 (0.57, 1.99) | 1.41 (0.78, 2.56) |
| 2 | 0.96 (0.50, 1.84) | 1.47 (0.80, 2.68) |
| 3 | 0.85 (0.43, 1.68) | 1.19 (0.63, 2.24) |
| 4 | 0.63 (0.28, 1.41) | 1.41 (0.73, 2.71) |
| 5–Least disadvantaged | Reference group | Reference group |
Residential remoteness
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Major cities | 1.06 (0.71, 1.60) | 1.12 (0.80, 1.57) |
| Outer regional | 0.84 (0.51, 1.37) | 1.32 (0.91, 1.90) |
| Remote | 0.89 (0.54, 1.48) | 0.89 (0.59, 1.34) |
| Very remote | 0.70 (0.43, 1.13) | 0.75 (0.49, 1.15) |
| Inner regional | Reference group | Reference group |
Maternal mental health contact b
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Yes | 0.92 (0.73, 1.17) | 1.44 (1.17, 1.76) |
| No | Reference group | Reference group |
Child has disability
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Yes | 1.53 (1.16, 2.03) | 1.27 (0.97, 1.66) |
| No | Reference group | Reference group |
Notes: a Adjusted for characteristics listed in table.
b Mother had a mental health diagnosis in HMDC or MHIS records that occurred prior to the child’s mental health contact.
c Bold text denotes statistically significant estimates where the 95 per cent CIs did not include the null value.
Personality disorder
Aboriginal and/or Torres Strait Islander
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Yes | 0.72 (0.45, 1.17) | 1.09 (0.96, 1.25) |
| No | Reference group | Reference group |
Sex
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Female | 2.00 (1.33, 3.00) c | 1.48 (1.33, 1.65) |
| Male | Reference group | Reference group |
Preterm
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| <37 weeks | 1.14 (0.66, 1.97) | 1.02 (0.85, 1.22) |
| >37 weeks | Reference group | Reference group |
Mother’s age at birth
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| <20 years | 0.98 (0.47, 2.04) | 0.99 (0.80, 1.24) |
| 20–29 years | 0.97 (0.53, 1.76) | 0.99 (0.85, 1.15) |
| 30–39 years | Reference group | Reference group |
| 40+ years | 1.56 (0.20, 12.03) | 1.42 (0.91, 2.21) |
Father’s age at birth
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| <20 years | 0.30 (0.06, 1.38) | 1.25 (0.94, 1.67) |
| 20–29 years | 1.21 (0.66, 2.20) | 1.11 (0.95, 1.29) |
| 30–39 years | Reference group | Reference group |
| 40+ years | 1.99 (0.76, 5.17) | 1.25 (0.98, 1.59) |
| Missing age | 1.55 (0.79, 3.04) | 1.21 (0.99, 1.48) |
Maternal marital status at birth
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Never married | 0.80 (0.50, 1.30) | 1.30 (1.12, 1.50) |
| Divorced/separated | Count too small | 1.63 (1.11, 2.39) |
| Unknown/not stated | 3.61 (0.87, 14.94) | 2.07 (1.10, 3.87) |
| Married/de facto/widowed | Reference group | Reference group |
Socioeconomic status
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| 1–Most disadvantaged | 1.44 (0.44, 4.75) | 1.14 (0.84, 1.55) |
| 2 | 1.36 (0.40, 4.62) | 1.06 (0.78, 1.46) |
| 3 | 0.96 (0.26, 3.53) | 1.02 (0.74, 1.42) |
| 4 | 1.87 (0.51, 6.82) | 0.92 (0.65, 1.32) |
| 5–Least disadvantaged | Reference group | Reference group |
Residential remoteness
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Major cities | 1.34 (0.60, 3.00) | 1.04 (0.87, 1.26) |
| Outer regional | 1.85 (0.77, 4.42) | 0.86 (0.69, 1.07) |
| Remote | 1.47 (0.57, 3.80) | 0.84 (0.66, 1.06) |
| Very remote | 1.04 (0.41, 2.63) | 0.79 (0.62, 1.00) |
| Inner regional | Reference group | Reference group |
Maternal mental health contact b
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Yes | 1.03 (0.69, 1.53) | 1.59 (1.42, 1.79) |
| No | Reference group | Reference group |
Child has disability
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Yes | 2.49 (1.62, 3.84) | 1.61 (1.39, 1.86) |
| No | Reference group | Reference group |
Notes: a Adjusted for characteristics listed in table.
b Mother had a mental health diagnosis in HMDC or MHIS records that occurred prior to the child’s mental health contact.
c Bold text denotes statistically significant estimates where the 95 per cent CIs did not include the null value.
Organic disorder
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
Aboriginal and/or Torres Strait Islander
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Yes | 1.36 (0.71, 2.60) | 0.88 (0.53, 1.47) |
| No | Reference group | Reference group |
Sex
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Female | 0.59 (0.33, 1.05) | 0.50 (0.32, 0.79) |
| Male | Reference group | Reference group |
Preterm
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| <37 weeks | 0.93 (0.41, 2.09) | 0.72 (0.31, 1.66) |
| >37 weeks | Reference group | Reference group |
Mother’s age at birth
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| <20 years | 0.42 (0.16, 1.13) | 2.30 (0.91, 5.82) |
| 20–29 years | 0.58 (0.28, 1.21) | 1.93 (1.04, 3.59) c |
| 30–39 years | Reference group | Reference group |
| 40+ years | Count too small | 3.65 (0.78, 17.03) |
Father’s age at birth
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| <20 years | 0.94 (0.22, 3.98) | 0.87 (0.28, 2.74) |
| 20–29 years | 1.01 (0.45, 2.29) | 0.89 (0.52, 1.51) |
| 30–39 years | Reference group | Reference group |
| 40+ years | 0.96 (0.21, 4.37) | 0.50 (0.14, 1.78) |
| Missing age | 1.55 (0.65, 3.71) | 0.60 (0.23, 1.52) |
Maternal marital status at birth
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Never married | 1.06 (0.56, 2.02) | 0.81 (0.42, 1.57) |
| Divorced/separated | 1.28 (0.30, 5.47) | 1.98 (0.48, 8.27) |
| Unknown/not stated | Count too small | Count too small |
| Married/de facto/widowed | Reference group | Reference group |
Socioeconomic status
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| 1–Most disadvantaged | 0.76 (0.22, 2.61) | 1.54 (0.36, 6.56) |
| 2 | 0.52 (0.14, 1.97) | 2.01 (0.47, 8.58) |
| 3 | 0.68 (0.18, 2.67) | 1.44 (0.32, 6.56) |
| 4 | 0.88 (0.21, 3.70) | 2.17 (0.47, 9.95) |
| 5–Least disadvantaged | Reference group | Reference group |
Residential remoteness
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Major cities | 1.70 (0.60, 4.84) | 1.41 (0.67, 2.99) |
| Outer regional | 0.44 (0.10, 1.97) | 1.09 (0.45, 2.63) |
| Remote | 0.71 (0.18, 2.75) | 0.56 (0.18, 1.75) |
| Very remote | 0.43 (0.11, 1.61) | 0.90 (0.32, 2.50) |
| Inner regional | Reference group | Reference group |
Maternal mental health contact b
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Yes | 0.75 (0.43, 1.32) | 1.29 (0.79, 2.11) |
| No | Reference group | Reference group |
Child has disability
| Characteristic | DFV exposure adjusted hazard ratios a (95% CI) | No DFV exposure adjusted hazard ratios a (95% CI) |
|---|---|---|
| Yes | 2.13 (1.17, 3.88) | 1.99 (1.19, 3.32) |
| No | Reference group | Reference group |
Notes: a Adjusted for characteristics listed in table.
b Mother had a mental health diagnosis in HMDC or MHIS records that occurred prior to the child’s mental health contact.
c Bold text denotes statistically significant estimates where the 95 per cent CIs did not include the null value.
Appendix D:
Adjusted hazard ratios and 95 per cent confidence intervals for the risk associated with DFV exposure on specific mental health diagnosis groups stratified by Aboriginal and Torres Strait Islander status
The tables below provide the adjusted hazard ratios and 95 per cent confidence intervals (CIs) for the risk associated with DFV exposure on specific mental health diagnosis groups (relating to Figures 8 and 9 in the report) for Aboriginal and Torres Strait Islander children and non-Aboriginal and Torres Strait Islander children. Individual models were run for each group. The first 10 tables provide information on Aboriginal and Torres Strait Islander children and the last 10 tables provide information on non-Aboriginal and Torres Strait Islander children. Adjustments were made for sex, early gestation (<37 weeks), mother’s age at birth, father’s age at birth, maternal marital status at birth, SES, residential remoteness, disability and maternal mental health contact. Bolded text in the tables denotes statistically significant estimates where the 95 per cent CIs did not include the null value.
Aboriginal and Torres Strait Islander children
Mental health contact with no diagnosis recorded
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 1.45 (1.34, 1.57) |
| No | Reference group |
Other mental illness-related contacts
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 1.07 (0.77, 1.51) |
| No | Reference group |
Intentional self-harm
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 1.67 (1.31, 2.15) |
| No | Reference group |
Substance use disorder
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 1.85 (1.52, 2.25) |
| No | Reference group |
Psychological development disorder
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 1.10 (0.95, 1.27) |
| No | Reference group |
Depressive disorder
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 1.30 (1.00, 1.70) |
| No | Reference group |
Anxiety
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 1.40 (1.25, 1.58) |
| No | Reference group |
Schizophrenia and psychoses
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 1.33 (1.09, 1.61) |
| No | Reference group |
Personality disorder
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 1.71 (0.96, 3.03) |
| No | Reference group |
Organic disorder
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 1.68 (1.02, 2.76) |
| No | Reference group |
Non-Aboriginal and Torres Strait Islander children
Mental health contact with no diagnosis recorded
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 1.56 (1.39, 1.75) |
| No | Reference group |
Other mental illness-related contacts
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 1.35 (0.90, 2.03) |
| No | Reference group |
Intentional self-harm
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 1.30 (0.90, 1.88) |
| No | Reference group |
Substance use disorder
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 2.48 (1.52, 4.05) |
| No | Reference group |
Psychological development disorder
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 1.22 (1.02, 1.45) |
| No | Reference group |
Depressive disorder
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 1.36 (0.99, 1.87) |
| No | Reference group |
Anxiety disorder
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 1.51 (1.31, 1.75) |
| No | Reference group |
Schizophrenia and psychoses
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 1.42 (1.09, 1.86) |
| No | Reference group |
Personality disorder
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 1.66 (0.95, 2.89) |
| No | Reference group |
Organic disorder
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 0.99 (0.55, 1.77) |
| No | Reference group |
Appendix E:
Adjusted hazard ratios and 95 per cent confidence intervals for the risk associated with DFV exposure on specific mental health diagnosis groups stratified by disability status
The tables below provide the adjusted hazard ratios and 95 per cent confidence intervals for the risk associated with DFV exposure on specific mental health diagnosis groups (relating to Figures 10 and 11 in the report) for children with disability and children with no disability. Individual models were run for each group. The first 10 tables provide information on children with disability and the last 10 tables provide information on children with no disability. Adjustments were made for Aboriginal and Torres Strait Islander status, sex, early gestation (<37 weeks), mother’s age at birth, father’s age at birth, maternal marital status at birth, SES, residential remoteness and maternal mental health contact. Bolded text in the table denotes statistically significant estimates where the 95 per cent CIs did not include the null value.
Child with disability
Mental health contact with no diagnosis recorded
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 1.59 (1.44, 1.77) |
| No | Reference group |
Other mental illness-related contacts
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 1.72 (1.55, 1.91) |
| No | Reference group |
Intentional self-harm
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 1.73 (1.56, 1.92) |
| No | Reference group |
Substance use disorder
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 1.72 (1.56, 1.91) |
| No | Reference group |
Psychological development disorder
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 1.53 (1.38, 1.71) |
| No | Reference group |
Depressive disorder
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 1.72 (1.55, 1.91) |
| No | Reference group |
Anxiety disorder
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 1.63 (1.47, 1.81) |
| No | Reference group |
Schizophrenia and psychoses
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 1.71 (1.54, 1.89) |
| No | Reference group |
Personality disorder
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 1.74 (1.57, 1.93) |
| No | Reference group |
Organic disorder
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 1.73 (1.57, 1.92) |
| No | Reference group |
Child with no disability
Mental health contact with no diagnosis recorded
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 1.88 (1.78, 1.98) |
| No | Reference group |
DFV exposure
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 2.03 (1.93, 2.14) |
| No | Reference group |
Intentional self-harm
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 2.02 (1.92, 2.13) |
| No | Reference group |
Substance use disorder
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 2.02 (1.92, 2.13) |
| No | Reference group |
Psychological development disorder
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 1.93 (1.83, 2.04) |
| No | Reference group |
Depressive disorder
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 2.02 (1.91, 2.12) |
| No | Reference group |
Anxiety disorder
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 1.92 (1.82, 2.03) |
| No | Reference group |
Schizophrenia and psychoses
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 2.00 (1.90, 2.11) |
| No | Reference group |
Personality disorder
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 2.05 (1.94, 2.16) |
| No | Reference group |
Organic disorder
| DFV exposure | Adjusted hazard ratio (95% CI) |
|---|---|
| Yes | 2.05 (1.94, 2.16) |
| No | Reference group |